|
|
Research Papers Indian Pediatrics 2007; 44:903-911 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Role of Paracetamol in Treatment of Childhood Fever: A Double-Blind Randomized Placebo Controlled Trial |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
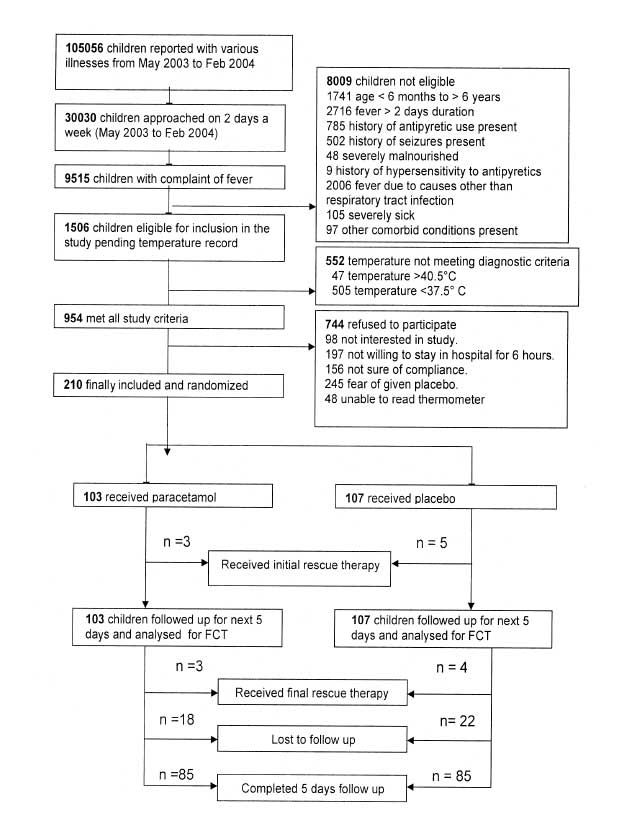
Beneficial effects of fever in disease are known since ancient times(1). Recent studies indicate that antipyretics in fever may actually prolong or worsen varicella, rhinovirus, and Plas-modium falciparum infections(2-5). A Cochrane review(6) has also concluded that the evidence supporting use of paracetamol–the most widely used over the counter drug used for treatment of childhood fever–to reduce fever in children is inconsistent and weak! We conducted a double blind randomized controlled trial to assess the role of paracetamol in treatment of fever associated with uncomplicated respiratory tract infections in children. We started with the hypotheses that (i) Use of paracetamol prolongs the fever clearance time (time between onset of treatment and return of temperature to normal) and (ii) The rate of fall of temperature following paracetamol administration is similar to placebo. Subjects and Methods The study was conducted at a tertiary care hospital over 1 year. Febrile children (age: 6 mo-6 yr; axillary temperature: 37.6-40.5ºC; duration of illness: less than 2 days) with a clinical diagnosis of uncomplicated acute respiratory tract infection (without cyanosis, convulsions, pneumothorax, empyema or respiratory failure were included. Children with personal or family history of seizures, neurological, hepatic or renal disease, peptic ulcer disease, tuberculosis, blood dyscrasia, malignancy, and immune suppression were excluded. Subjects with severe malnutrition(7) and known hyper-sensitivity to NSAIDs were not enrolled. Patients with history of administration of antipyretic or antibiotics within last 2 days were also excluded. Informed consent was obtained from the eligible participants. The study was approved by the Institutional Research Board including the ethical clearance. Randomization and blinding: Simple randomization was done using random number table. The bottles were coded from A to J using the random number table. Five of the 10 alphabets used were randomly allocated to paracetamol or placebo group. A set of ten codes was used to minimize guessing of code by the investigator. The subject received the similarly coded bottle throughout the study period. The randomization coding and labelling was done at hospital pharmacy and the code master list was opened up only at the end of statistical analysis. The participants, investigators and observers were blinded to group assignment. The drug and placebo were made to look, smell and taste similar. Intervention and monitoring: Baseline information was obtained on anthropometry, presenting symptoms, and duration of fever. The elixir was given in a dose of 0.6 mL/kg (15 mg/kg body weight of paracetamol) immediately after recording the temperature. The dose was repeated immediately if the child vomited the drug within 15 minutes of administration, or after 6 hrs, if the axillary temper-ature was ³37.6ºC. The temperature was recorded by placing the bulb of a pre-standardized thermometer at apex of axilla between anterior and posterior axillary folds for 5 minutes at 0 hour, 30 minutes, and then hourly for 6 hours. All the subjects were hospitalized for a minimum of 8 hours in a general ward without the facility of air conditioning; thereafter, the duration of stay in hospital depended on the general condition. All the temperature readings during first six hours of hospitalization were taken by one of the investigator (HG). Thereafter, the temperature recording was done at home or hospital (for admitted patients) at 6 hourly intervals and when-ever considered necessary by parents/observer. For home monitoring, parents were provided a pre-standardized thermometer by the investigator and trained in the method of measuring temperature. The syrup containing paracetamol or placebo was given in a dose of 0.6 mL/kg by the parents whenever the temperature was ³37.6ºC. Parents or guardians maintained a record of temperature and the time of consumption of doses in a small diary. Parents were asked to avoid other pharmacological or physical methods of antipyresis including hydrotherapy. Treatment and monitoring continued every 6 hrs. till the defined end point of study i.e., temperature returning to normal ³37.5ºC (axillary) and remaining so for 24 hours; or 5 days after enrolment, whichever was earlier. Subjective improvement was noted for 6 separate items (activity, alertness, mood, comfort, appetite and fluid intake) during the initial 6 hours following recruitment, on a 5 point likert scale. Monitoring was also done for the following adverse effects: Hypothermia, headache, vomiting and abdominal pain. Any occurrence of seizure was also recorded. Rescue therapy in the form of ibuprofen and/or sponging was given if the child had a febrile seizure, or axillary temperature increased to >40.5ºC. Decisions regarding other aspects of management including antimicrobial therapy were taken by the attending physician. A 2 mL venous blood sample was collected in first 103 subjects at the beginning and end point of the study, for measuring liver enzymes. Outcome variables: Fever clearance time (time between onset of treatment to return of temperature to normal i.e., £37.5°C) was the primary outcome measure. Secondary outcome measures included (i) rate of fall of temperature; (ii) percent reduction of temperature; (iii) proportion of afebrile children at 1, 2, 4 and 6 hours; (iv) symptomatic improvement (based on categorical improvement in activity, alertness, mood, comfort, appetite and fluid intake), and (v) clinical and biochemical (liver enzymes) adverse drug effects. Statistical methods: A sample size of 168 (84 in each group) was calculated to be adequate to detect a mean difference of 12 hours (SD = 24 hr) in fever clearance time with type I error of 0.05 and 90% power(8). One sample Kolmogorov-Smirnov test was used to investigate normal distribution of fever clearance time and rate of fall of temperature. Kaplan Meier Survival analysis was performed to estimate the median fever clearance time. Rate of fall (ROF) of temperature was analysed by analysis of variance for repeated measures (MANOVA). All other means were compared by Student’s t test or one way ANOVA; and proportions by Chi-square or Fisher exact test. The level of significance for all tests was 0.05. Analysis was conducted using the SPSS version 10.0 software. Results Of 954 children fulfilling the eligibility criteria, 210 febrile children were finally randomized to receive either paracetamol (n = 103) or placebo (n = 107) therapy (Fig. 1).
Numbers of children in age categories of 6 months to 1 year, 1 year to 3 years and 3 years to 6 years, were 27 (26%) vs 28 (26%), 55 (53%) vs 52 (49%) and 21 (20%) vs 27 (25%) in the paracetamol and placebo groups, respectively. Almost all children in the two groups had a body weight of >80%, and height >95% of the expected for age (CDC Reference Charts 2001)(9). The initial temperature at enrolment was between 37.6-38.5ºC in 42 (41%) subjects in the paracetamol group as compared to 49 (46%) in the placebo group. Temperatures between 38.6ºC to 39.5ºC were recorded in 28 (27%) and 36 (34%) in paracetamol and placebo groups, respectively. Thirty three (32%) children in the paracetamol group and 22 (21%) in the placebo group had temperature above 39.5ºC. These differences were statistically not significant (P >0.05). The baseline characteristics of enrolled subjects with respect to age and sex distribution, nutritional status, maternal educational status, morbidity profile, and temperature at enrolment were comparable between the two groups (Table I). The number of subjects with clinical diagnoses of Pneumonia [cough and fever with presence of fast breathing or chest indrawing as per World Health Organization definition(10)], URTI (cough and fever with no chest indrawing or fast breathing) or wheeze associated respiratory tract infections (Pneumonia or URTI associated with audible or auscultable wheeze) were also comparable between the two groups (Table I). TABLE I Comparison of Baseline Characteristics of the Subjects in Paracetamol and Placebo Groups
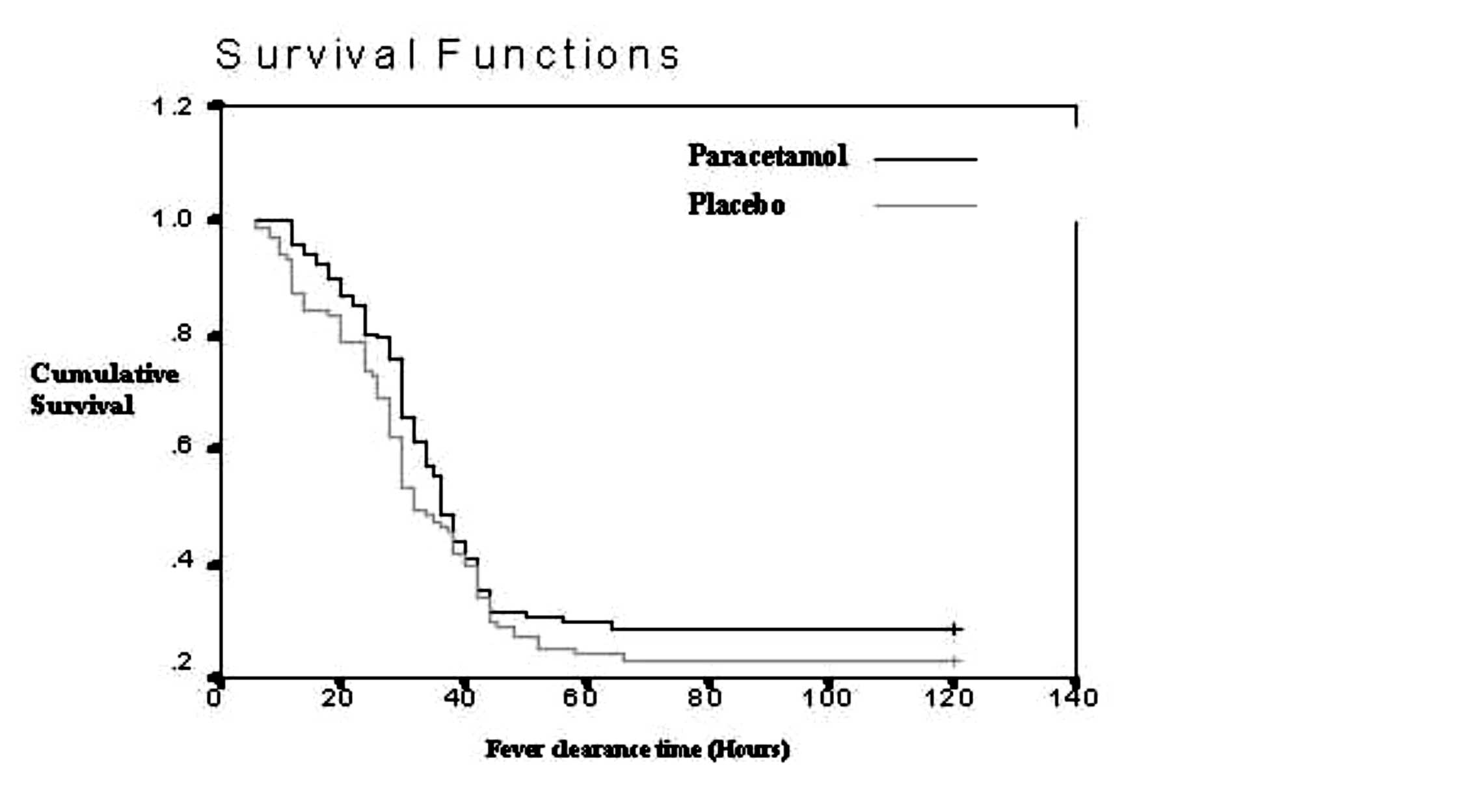
Figures in parentheses indicate percentages. URTI: Upper respiratory tract infection; WRTI: Wheeze associated respiratory tract infection. Fever clearance time (FCT): The median fever clearance time (SE, 95% CI) was 32 (2, 22-37) hours in the paracetamol group as compared to 36 (1, 33-39) hours in placebo group (P = 0.23). Mean difference between the groups was 2.1 hrs (95% CI: 1.6 to 5.8; P = 0.26). Figure 2 shows the FCT in the two groups as a survival curve by Kaplan Meier analysis.
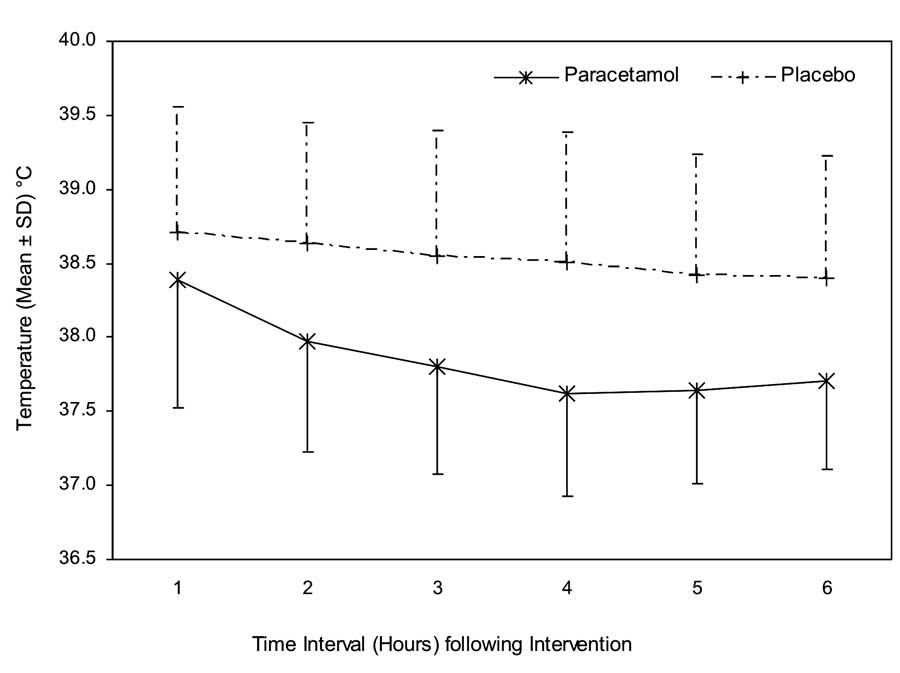
Reduction in temperature: Group wise distribution of ROF of temperature was found to be Gaussian. The ROF in the first 6 hours after drug administration was significantly higher (P <0.001) in the paracetamol group (0.20 ± 0.11ºC/h) as compared to placebo (0.05 ± 0.08ºC/h). The mean ROF was significantly higher (P <0.001) at all time point intervals (1, 2, 3, 4, 5 and 6 hours) in the paracetamol group (0.89, 0.54, 0.39, 0.33, 0.25 and 0.20) as compared to placebo (0.21, 0.10, 0.08, 0.07, 0.06 and 0.05), respectively. The mean difference in the ROF between the two groups was maximum at 1 hour (0.68; 95% CI 0.81 to 0.54) after initiation of treatment; and minimum after 6 hours of drug administration. The overall differences between and within the groups were highly significant (P <0.001). Figure 3 depicts mean (SD) hourly temper-atures at different time intervals after intervention in the paracetamol and placebo groups. Table II shows percentage reduction (mean ± SD) of temperature at different time point intervals in paracetamol and placebo groups. Percent reduction was higher in paracetamol group as compared to placebo group at 2, 4 and 6 hours after initiation of therapy. Maximum and minimum mean difference between the groups was noticed at 4 and 6 hours, respectively. Mean percent reduction in the paracetamol group was 1.5 to 2.5 times more as compared to the placebo. TABLE II Percentage Reduction in Temperature at 2, 4 and 6 Hours in Paracetamol and Placebo Groups after Intervention
All values mean + SD. Proportion of afebrile children was consistently more in the paracetamol as compared to placebo group (16% vs. 1%; 26% vs 3%; 47% vs 13% and 49% vs 17% at 1, 2, 4 and 6 hours, respectively (P <0.001). Maximum difference between the two groups was seen at 1 and 2 hours after intervention. Only 2 children became afebrile between 4 to 6 hours in the paracetamol group. Subjective improvement: Table III shows the subjective improvement by at least one category in each of the 6 parameters at 4 and 6 hours after initiation of treatment. Number of children showing improvement was significantly higher in the paracetamol group at 6 hours. The improvement was maximum in activity and alertness, moderate in mood and comfort; and least in appetite and fluid intake. TABLE III Number of Children having Atleast one Category Improvement from Baseline in Paracetamol and Placebo Groups after Intervention
Figures in parentheses indicate percentages. Adverse events: Nine children in the paracetamol group had adverse effects as compared to none in the placebo group during first 6 hours. Mild gastro-intestinal symptoms including pain abdomen, vomiting and nausea were observed in 8 children; one child had severe headache unrelated to the degree of temperature. None of the adverse effects was severe enough to necessitate cessation of therapy. No child had a febrile seizure. The mean value of liver enzymes was comparable between the groups, both at the beginning and end of the study. Also, the difference from the respective baseline value was not significant in both the groups (Table IV). TABLE IV Liver Function in the Two Groups Before and After Therapy
All P values <0.05; All values mean + SD. Rescue therapy was needed in 8 patients (paracetamol-3; placebo-5) during the first 6 hours after administration of the drug. Another 7 subjects (paracetamol-3; placebo-4) required rescue therapy on subsequent home monitoring. Proportion of children receiving antibiotics was comparable in the two groups [paracetamol: 24% (n = 25) vs placebo: 22% (n = 24); P = 0.75]. Discussion This trial attempted to generate data on effect of paracetamol on overall duration of fever and its antipyretic efficacy over placebo in a randomized controlled manner. The study evaluated functionally important outcomes such as overall duration of fever and improvement in overall symptomatology. Results on Fever Clearance Time in the present study negated our working hypothesis that administration of paracetamol in febrile children increases the overall duration of febrile episode by impairing the beneficial effect of raised body temperature in augmenting the host immune response. Simultaneously, these results suggested that there is no overall benefit/harm of paracetamol therapy in altering the course of disease in pediatric respiratory tract infections. Kramer, et al.(11), in a study on 304 febrile children, also reported that the mean fever clearance time was not different with paracetamol or placebo administration. This study, however, had methodological concerns such as unusually long enrolment period (8 years), changes in study site and personnel besides a high drop-out rate. Although the follow-up loss was also high in our group (24%), adequacy of sample size despite the follow-up loss and use of survival analysis in our study improve the validity of the results. Another shortcoming was that the present study could only evaluate the effect of paracetamol on overall duration of fever when it was a part of uncomplicated respiratory infections which may not be generalizable to other infections. In another investigation of fever clearance time in children suffering from Plasmodium falciparum malaria, no significant difference in FCT could be documented with paracetamol(5). However, the sample size was inadequate to draw valid conclusions. Although, there was no effect of paracetamol administration on overall duration of fever, it was superior to placebo in terms of rate of fall of temperature, proportion of afebrile children and symptomatic improvement in activity, alertness, mood and comfort. The maximum effect of paracetamol was observed during the first hour after drug administration, both in terms of reduction of temperature and proportion of afebrile children. Time course effect in the paracetamol group (Fig. 3) showed declining mean temperatures till 4 hours, followed by an upward trend to 6 hours. The difference between the two groups was minimum between 5 to 6 hours, though it was still significant. This can be explained due to waning drug levels in plasma (half-life = 2 hours) at this time. The pattern of time course effect in placebo group was not consistent. These findings suggest that paracetamol in a dose of 15 mg/kg is an effective antipyretic and the effect lasts up to 6 hours. The effect is maximum during the first hour and starts waning after 4 hours. Thus, a repeat dose, if required, is best administered 4 hours after the first dose. This clinical observation is in conformity with the dynamics and kinetics of paracetamol(12) and earlier reports(13).
Hunter, et al.(14) in 1973 examined ROF for 2 hours following administration of paracetamol (5-10 mg/kg) or placebo in 67 children having fever. The ROF (ºC/h) in paracetamol and placebo groups were 0.6 vs 0.1, 1.1 vs 0.6, 1.5 vs 0.5, and 1.6 vs 0.5 at 0.5, 1, 1.5 and 2 hours, respectively. The corresponding ROF in the paracetamol group was lower in our study except at 1 hour. The difference can be attributed to higher baseline temperature (>39.5ºC) in the Hunter study, as it is known that higher initial temperature show a greater decline in temperatures after antipyretic administration than lower baseline temperatures(15). Studies to compare the rate of fall (ROF) of temperature up to 6 hours after administration of paracetamol are not available. Our study did not find any significant adverse reaction with administration of paracetamol in therapeutic doses (15 mg/Kg) for short period. However, the study lacked adequate power to validly comment on this outcome. Meta-analysis of data from three trials(15-17) involving a total of 254 participants showed that the incidence of adverse events in the paracetamol (9/130) and placebo (4/124) groups did not differ significantly. Adverse events were mild in all cases and included drowsiness and mild gastrointestinal symptoms. Thus, paracetamol can be considered to be a safe drug at therapeutic levels. Overall the results of our study showed that paracetamol achieves effective antipyresis and provides early symptomatic improvement without increasing the duration of fever as compared to placebo in children with respiratory tract infections. Adverse effects are minimum. In view of these results, we advocate to continue the practice of using paracetamol for intermittent antipyresis in children having acute respiratory tract infections. Contributors: PG and DS conceptualized the study and its design. HG collected the data and drafted the initial version of manuscript. The manuscript was modified by DS and PG. All authors participated in analysis and interpretation of data and the final approval of manuscript. DS will act as the guarantor. Competing Interests: None. The drug and placebo were packaged and dispensed at the pharmacology department of the institute without any grant, free supply or sponsorship from pharmaceutical companies. Funding: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()