|
|
Brief Reports Indian Pediatrics 2006;43:1070-1075 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
A Comparative Study of Non-Pharmacological Methods to Reduce Pain in Neonates |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Sheila Mathai, Nisha Natrajan and N.R. Rajalakshmi From the Department of Pediatrics, AFMC, Pune 411 040; and INHS Asvini, Colaba, Mumbai 400 005, India. Correspondence to: Surg Cdr Sheila Mathai, Associate Professor, Department of Pediatrics, Armed Forces Medical College, Pune 411 040, India. E-mail: [email protected] Manuscript received: June 27, 2005; Initial review
completed: September 20, 2005;
Despite an increasing awareness regarding pain in neonates and its detrimental effect on neurobehavioral development(1,2), newborns continue to be subjected to procedural pain without analgesia. Lack of adequate training of health care personnel, the inability of neonates to express themselves and fear of the side effects of analgesics are some of the reasons why this happens(3). Pain perception is associated with physiological and complex behavioral changes in neonates in the form of immediate alteration in state of arousal, disruption of adaptation to the environment and changes in vital parameters. Crying and changes in facial expression are common manifestations of pain(4). Heel prick, for capillary sampling, is one of the most frequently performed procedures in the neonatal nursery and postnatal ward. The sharp, acute pain that it produces is more than that of a vene-puncture and can be very distressing to the neonate(5). In the past few years there have been a number of studies to determine simple measures to reduce pain in neonates. Non-pharmacological methods are feasible, accept-able and easy to use. Though they have all shown promise, no single method is universally recommended. This study was done to objectively compare some of these methods with the intention of deciding which was the best one to incorporate into the Unit’s policy on pain management. Subjects and Methods (a) The study was carried out in the Transitional Care Unit and Postnatal Ward of a large, teaching hospital. This was a randomized study on 104 term neonates, who underwent heel prick for collection of blood for bilirubin estimation. Term babies older than 24 hrs of life were included. Those excluded were babies <2 Kg sick babies with unstable vitals or on IV fluids, oxygen or any drugs requiring resuscitation at birth, with neurological abnormalities, or having major congenital defects. Outcome variables (a) Time of first cry (till the baby took the first inspiration after starting to cry) and total duration of cry were measured after the stimulus. (b) Heart rate and SpO2 were recorded before giving the stimulus and at 2 and 4 minutes after the stimulus. (c) DAN score was assessed before giving the stimulus and again at 30 sec, 1 min, 2 min and 4 min after the stimulus. Sample size estimation Sample size was calculated to show a decrease of at least 20% in the mean DAN score after any intervention compared with no intervention. Randomization Subjects were randomized (using random number table) to receive one of the following 6 interventions: Expressed Breast Milk (EBM); Sucrose (20% S); Distilled Water (DW); Non Nutritive Sucking (NNS); Massaging (M); and Rocking (R). Intervention Parents were explained the procedure and informed consent was taken. The baby was placed naked in a cot under a radiant warmer in a quiet, diffusely lighted room. The pulse oximeter probe was attached firmly to the hand. All interventions were kept ready for every baby. Blinding was achieved by one of the observors (Observor 1) leaving the bedside at this stage and standing behind a screen. The baby was then assigned to one of the groups. A trained nurse gave the selected intervention two minutes before the heel prick as follows: EBM, 20% sucrose or distilled water were administered (2ML) in the baby’s mouth with a dropper. In NNS group, a sterile pacifier (standard silicone pacifier) was held gently in the neonate’s mouth and the palate tickled to stimulate sucking. This was continued during and up till 2 minutes after the heel prick. In M group, neonates were subjected to firm, gentle stroking with bare fingers in a rhythmical manner starting from the forehead and going down to the chest, arms and legs. 6 strokes were given in each area and these were continued in a cyclical manner during and up till 2 minutes after the heel prick. In R group, neonates were rocked by lifting the baby’s head off the cot on the palm of the hand (without lifting the body off the cot) and making rocking movements in a gentle, rhythmic manner. This was continued during and up till 2 minutes after the heel prick. Data Collection Two minutes after commencement of the intervention, just before the heel prick, Observor 2 evaluated the Prechtl’s State of arousal, HR and SpO2. Baseline DAN score (Table I) was also recorded. A trained nurse then gave the heel prick in a standard manner with a lancet. Three nurses who were trained in giving effective heel pricks did the sampling all through the study. Squeezing was done not more than 3 times to collect the sample. The duration of first cry (time to first inspiration after commencement of cry) and total duration of cry were recorded by Observor 1 who was blinded to the intervention. Observor 2, who was not blinded, assessed the DAN score again at 30 sec, 1 min, 2 min and 4 min after the prick. Heart rate and SpO2 were also recorded from the pulse oximeter at 2 and 4 minutes. TABLE I Douleur Aiguë du Nouveau-né (DAN) Behavioral Scale
Statistical analysis Data was analyzed using SPSS ver 11.5. ANOVA followed by Fischer’s exact ‘t’ test where required. Multivariate analysis was used for demographic data. Pearson’s correlation test was used where required. Table II Demographic Characteristics of Different Groups (± 2 SD)
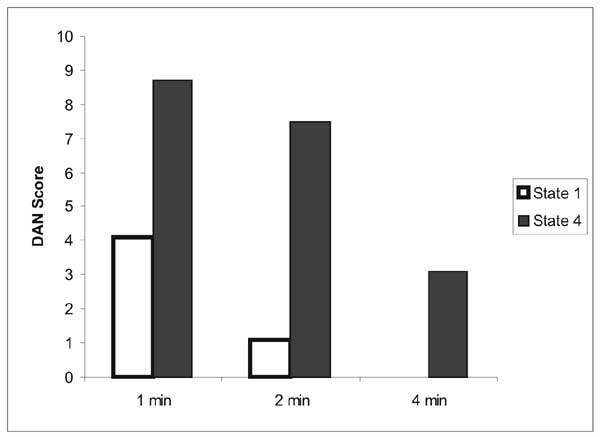
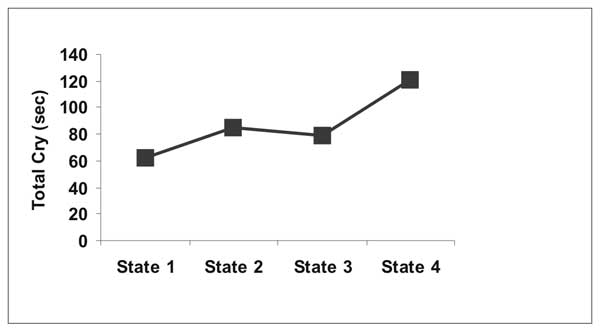
Results The demographic characteristics were similar in all the groups (Table II). When DAN scores were compared, this was lowest at 30 sec in the sucrose group but was not sustained at 2 and 4 minute. At these times the scores were lowest in the NNS and rocking groups (Table III). The total duration of cry was lowest in these two groups as well (Table IV). There was no significant difference in physiological parameters between the groups. As regards the state of arousal, babies in states 1 and 2 showed significantly lower pain scores at all times (Fig.1). Duration of cry also correlated well with state of arousal at the time of painful stimulus. States of arousal >2 were associated with longer duration of cry (Fig. 2) as compared with states 1 and 2. TABLE III DAN Scores Before and After Heel Prick (± 2SD)
* Significant difference. Table IV Time of First Cry and Total Duration of Cry in Different Groups
* Significant difference.
Discussion Our study was a randomized, partially blinded study to compare the analgesic effects of common, non-pharmacological methods to reduce pain in neonates. Complete blinding was not possible as many of the interventions had to be continued during and after the painful stimulus. A number of studies have compared the effects of sucrose with other non-pharmacological methods of pain assess-ment(6,7). The Cochrane analysis suggests that sucrose is better than placebo in reducing the effects of painful stimuli(8). Some studies have found sucrose to be superior to EBM(9). Carbajal et al(10) have shown that pacifiers alone are better than sucrose(10). Other studies have shown that multimodal stimulation is better than just sucrose(11). Rocking and pacifiers (NNS) have been compared and both have been found to reduce crying(12). Studies have also shown that NNS reduces the stress of pain(13). Our study showed that rocking or NNS were more effective than DW, EBM, massage or sucrose in reducing the DAN score at 2 and 4 minutes after the painful stimulus. Breastfeeding has been found to be analgesic and this is probably due to the multimodal stimulation that a neonate experiences when suckling from the breast compared to EBM alone(14). An interesting finding in our study is that state of arousal of the baby at the time of the painful stimulus was found to affect pain scores with babies in the sleep state (states 1 and 2) showing lower scores and a shorter duration of crying as compared to those in higher states (states 3,4). Some other authors have also reported similar findings(4,15). In conclusion our study suggests that rocking or giving a baby a pacifier are effective analgesics for the pain of heel pricks in stable, term neonates. Calming a baby into a sleeping state before a painful procedure may also decrease the response to pain. Contributors: SM conceived, designed and supervised the study, NN did the DAN scores and compiled the data, RL did the assessment of crying and helped in the collection of data and logistics. SM will act as guarantor for the manuscript. Funding: None. Competing interests: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
![]()