|
|
Case Reports Indian Pediatrics 2002; 39:1159-1161 |
||
|
Congenital Contractural Arachnodactyly (Beals Syndrome): First Case Report with Hypospadias |
||
|
Bhaskar Gupta
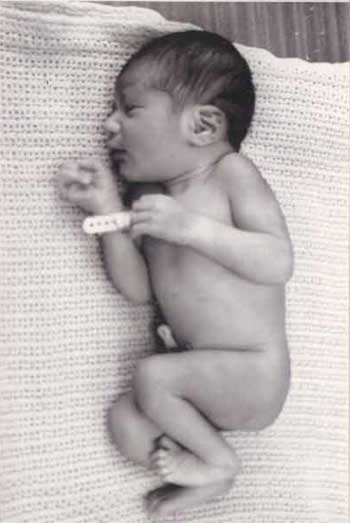
Congenital contractural arachnodactyly (Beals syndrome) is a rare autosomal dominant disorder caused by mutation in fibrillin 2 (FBN2) gene that is phenotypically similar to but less severe than Marfan syndrome. It is characterized by normal facies, arachnodactyly, dolichostenomelia, scoliosis, multiple joint contractures, limited extension of fingers and toes, camptodactyly with ulnar deviation of hands, hypoplasia of calf muscles, crumpled ears and congenital heart disease(1,2). With time there is spontaenous improvement in joint contractures but kyphosis tends to be progressive. Neonatal form results from new mutations and tends to be severe(3). Apart from its classical features, Beals syndrome may be associated with rare anomalies of eye, duodenum, pancreas and mental retardation, but associated genital anomalies in a male child have not been described yet. This is first case report of an association of Beals syndrome and coronal hypospadias. Case Report A full term appropriate for gestational age male neonate was born by emergency LSCS for fetal distress and oligohydramnios at a tertiary care hospital in Muscat, Sultanate of Oman to 18 years old primigravida mother. There was no history of consanguinity and any affected family members with congenital contractural arachnodactyly. The baby weighed 3000 g, and had a head circumference of 34 cm and length of 52 cm. On examination neonate had normal facies, high arched palate, long hands and feets (arachnodactyly), joint contractures of knee and elbows, long and slim limbs (dolichostenomelia), hypoplasia of calf muscles, crumpled ears (Fig. 1), camtodactyly with ulnar deviation of hands and coronal hypospadias with hooded prepuce, normal scrotum and testis. In addition to this the baby was noted to have a short systolic cardiac murmur on 3rd day of life. This baby had an uneventful course during the stay in hospital and was discharged after 3 days from the hospital. Ultrasound of abdomen revealed normal liver, spleen and kidneys. X-ray revealed long bones, widening of knee joints and normal skull, spine and pelvis. Eye examination showed normal lens and fundus.
Discussion Beals syndrome is phenotypically similar to Marfan syndrome and was originally described by Beals and Hecht in 1971(4). The detection rate of Beals syndrome has increased with the techniques of chromosomal localization, fluorescent in situ hybridization, isolation and mapping of FBN1 and FBN2 gene and its mutations(5). Arachnodactyly, flexion contractures and high arched palate may be seen as manifestations of neonatal Marfan syndrome which has striking phenotypic resemblance to Beals syndrome. However, significant cardiovascular and ocular manifestations are not found in Beals syndrome. The cardiac associations with Beals syndrome has been reported in various studies and may be present in 32% of cases, usually atrial septal defect or a ventricular defect unlike the structural cardiac defects in the form of aortic regurgitation, aortic dissection and dilatation of ascending aorta seen in 80% cases of Marfan syndrome. The characteristic association of ear abnormalities and hypoplasia of calf muscles seen in Beals syndrome also distinguishes it from Marfan syndrome(6). The crumpled ear which is a hallmark of Beals syndrome could be explained by the difference in expression of FBN1 and FBN2 gene in human ear cartilage. Fibrillin 1 provides the major structural function of the elastin associated microfibrils responsible for the manifestations of Beals syndrome(7-8).
This baby apart from all the features of Beals syndrome had additional coronal hypospadias. Only one such case has been reported earlier(9) in a girl with Beals syndrome who presented with ambiguous genitalia. Many such rare associations like ankyloblepharon, downslanting eyes, duodenal atresia, annular pancreas, female external genital anomalies have been described along with Beals syndrome. No specific etiopathological factors are incriminated. There is a varying severity in phenotypic presentation of Beals syndrome even among family members. The disease usually runs a benign course and with time there is spontaneous improvement of joint contractures, but kyphosis and scoliosis which is seen in 50% cases tends to be progressive(2,4). These children will need orthopedic management. Long term outcome of Beals syndrome is good as there is spontaneous improvement in joint contractures and with proper orthopedic management life span may be normal. Anesthetists should be made aware of the joint contractures and reduced mandible mobility and difficulty in intubation(10). Prenatal diagnosis may be offered to affected families. Contributors: BG worked up the child and wrote the manuscript. Funding: None. Competing interests: None stated.
| ||
|
References | ||
|
![]()