|
|
Case Reports Indian Pediatrics 2002; 39:1149-1152 |
||
|
Restrictive Dermopathy - A Case Report |
||
|
B. Mahadevan K. Karthikeyan* B. Vishnu Bhat D.M. Thappa*
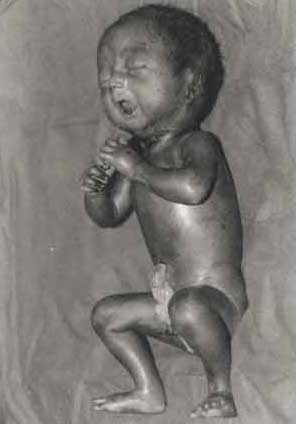
Restrictive dermopathy (RD) is one of the lethal forms of autosomal recessive skin dysplasia(1). This was first described by Witt et al.(2) in 1986 as a syndrome characterized by rigid or thick skin involving the entire body, dysmorphic facies, arthrogryposis multiplex and pulmonary hypoplasia. It is a rare disorder and only few cases have been reported in the literature(3). Here we report a case of restrictive dermopathy in a preterm newborn. Case Report The female newborn was born to non-consanguineous parents at 32 weeks of gestation by spontaneous vaginal delivery to a 26 years old second gravida mother. The present pregnancy was complicated by pregnancy induced hypertension. Ultrasono-gram at 31 weeks of gestation revealed intrauterine growth retardation and polyhydramnios. The newborn had an apgar score 4 at 1 minute and 5 at 10 minutes and required active resuscitation. On examination, the infant had characteristic facies with pinched nose, open mouth and micrognathia. The ears were low set. The birth weight was 1.2 kg, head circumference 27.5 cm and the crown-heel length 25.5 cm. The skin of the entire body was shiny and taut with prominent veins on the trunk. The mouth was small and locked in an open position. The cheeks were full and prominent. The nipple and areola were prominent. The skin was fissured at the flexures and erosive ulcers were seen at the pressure sites. The fingers were short, thin, and fixed in partial flexion. Hands and feet were edematous. Ankylosis was observed at hip, knee, ankle, shoulder, elbow, wrist and interphalangeal joints (Fig.1) Blood biochemistry did not reveal any abnormalities. Her hemogram was normal. Her VDRL, ANA and ELISA for HIV antibodies were negative. Serum calcium was normal and blood culture was sterile. Skiagram of chest revealed thin cortex with poor mineralisation of long bones. The lateral end of clavicle was hypoplastic. The ribs were slender and irregular. Echocardiogram was normal. Histopathological examination of the representative skin revealed normal epidermis. The dermis showed dense bands of collagen fibers oriented parallel to epidermis. Further, sebaceous and eccrine glands were reduced in number. Hair follicles were not visualized in the specimen. Elastin was absent in the dermis indicated by negative staining for elastin. Baby was given intravenous fluids, antibiotics and oxygen by hood initially followed by intragastric feedings. She expired on tenth day due to respiratory insufficiency. Discussion Restrictive dermopathy (RD) is characterized by abnormal facies, tight skin and secondary joint changes that are diagnostic(1). The skin is shiny and taut. The face is typical with a small, fixed and round open mouth, micrognathia, small nose and widely set ears(1,3). The face is expressionless with blurring of groove between nose and cheek and sparse or absent eyelashes, best described as ‘Asiatic porcelain doll"(1). Nipple and superficial vasculature are prominent because of atrophic epidermis. The skin may be fissured and eroded because of its rigidity. The nails may be short or very long and may be discolored or hypoplastic. Histopathological features include hyperkeratosis, parakeratosis and abnormal keratohyaline granules. The dermoepidermal junction is flat with complete lack of rete ridges. The dermis is thin with dense, thin collagen fibers parallel with epidermis, resembling in a scar or tendon and subcutis is thick with hypoplastic eccrine and sebaceous glands. The elastin fibers are absent in dermis(4,5). The other salient feature is multiple joint contractures (arthrogryposis)(3). The clavicles are thin and dysplastic. Pulmonary hypoplasia can occur in these patients and is usually fatal. The other rare features include premature teeth, choanal atresia, submucous cleft palate, hypospadias, urethral duplication, adrenal hypoplasia, patent ductus arteriosus, artrial septal defect and rocker bottom feet(2).
The pathogenesis of this disorder is probably due to skin dysplasia leading to a ‘Fatal Hypokinesia Deformation Sequence’(1). Limitation of movements at joints leads to contractures and in the chest result in pulmonary hypoplasia. Deficient fetal swallowing results in polyhydramnios and further decreased movements may also lead to a short umbilical cord(1,6). The neonatal history of this disorder is typical. Pregnancy is frequently abnromal with polyhydramnios, premature rupture of membranes, decreased fetal activity and fetal distress. Prematurity is the rule with majority of the affected individuals being still born. A few are alive at birth but most of the survivors die within the first week. The longest period of survival has been 120 days(3). Our patient survived for 10 days. Though rigid skin is a characteristic feature of RD, several disorders can present with rigid skin like sclerema neonatorum, scleredema, progressive familial scleroderma, syndesmodysplastic dwarfism and parana hard skin syndrome(2). However, they can be well delineated by their clinical and dermatopathological features. RD has to be differentiated from stiff skin syndrome and stiff baby syndrome. Stiff skin syndrome is characterized by generalized thickening of skin, in contrast to RD where usually dermis is thinned out. Hereditary stiff baby syndrome is a muscular disease characterized by attack of stiffness precipitated by surprise or physical contact(7). The other syndromes characterized by growth retardation, arthrogryposis, unusual facies and short life span include Pena- Shokier syndrome, cerebro-oculo-facio-skeletal syndrome COFS), Neu-Laxova syndrome and lethal multiple pterygium syndrome(1). Penna-Shokeir syndrome is associated with craniofacial abnormalities, multiple ankylosis and pulmonary hypoplasia but the skin is normal. Cerebro-oculo-facio skeletal syndrome and Neu-Laxova syndrome result due to fetal akinesia deformation sequence. In contrast to RD, these forms of fetal akinesia occur due to primary defect of the central nervous system. They are associated with microcephaly or absence of anterior horn cells in the spinal cord. RD is different from the above disorder as it results exclusively from skin disease(1,8) Prenatal diagnosis of RD may be possible by direct examination and biochemical analysis of fetal cells(1,2). RD is rare and our case is the first to be reported from Indian subcontinent. Contributors: BMD and BVB were responsible for the neonatal workup. DMT and KKN did the dermatological workup. BMD and KKN drafted the manuscript. DMT and BVB critically reviewed the manuscript. Funding: None. Competing interests: None stated.
| ||
|
References | ||
|
![]()