|
|
Brief Reports Indian Pediatrics 2002; 39:1138-1142 |
||
|
Laparoscopy in Diagnosis of Prolonged Neonatal Jaundice |
||
|
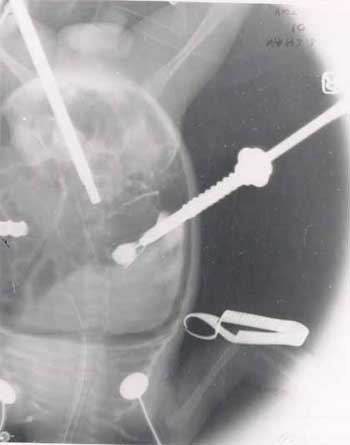
Prolonged neonatal jaundice may be caused by much different medical and surgical pathology. Jaundice persisting for more than 14 days postnatally is considered pathological and when more than 20% of the total bilirubin is direct, surgical causes should be excluded. Direct hyperbilirubinemia can be caused by many medical and surgical disorders and an early definitive diagnosis is an important step because the success rate of the operation performed in extra hepatic biliary atresia (EHBA) is inversely proportional to the age of the patient(1). The use of conventional investigations to differentiate medical causes of jaundice from biliary atresia is on many occasions unsuccessful, and surgical exploration may be needed. In the era of laparoscopy, this exploration can be omitted and replaced by a minimal invasive procedure that will help in diagnosis with a less risk for this group of patients. In the present report, the value of diagnostic laparoscopy and laparoscopic cholangiography in obstructive jaundice will be presented. Subjects and Methods Over a period of eight months, six patients with conjugated hyperbilirubinemia referred to the Department of Pediatric Surgery, V.S. Hospital, Ahmedabad were included. All the patients had direct bilirubin more than 20% of the total bilirubin level and underwent workup to diagnose various disorders causing conjugated hyperbilirubinemia including a liver biopsy. HIDA scan was done in two patients. All reports suggested of extra hepatic biliary atresia as a possible cause of the conjugated hyperbilirubinemia. Diagnostic laparoscopy was performed in all the patients and laparoscopic cholangiography was performed for documentation of the presence and patency of the extra hepatic and intrahepatic biliary tree. Veress needle was introduced into the abdominal cavity through an infraumbilical stab incision under general anesthesia and a pneumoperitoneum with a pressure of 6-8 mm Hg was created by CO2 insufflation. A 3 mm trocar was introduced into the abdominal cavity through the infraumbilical incision. The liver surface of infants with EHBA was greenish brown in color, coarse, irregular, firm and with a rounded inferior edge. The gallbladder was fibrotic or atretic. On the other hand, presence of a smooth, chocolate brown liver with a sharp edge was seen in patients with neonatal hepatitis. When the gall bladder was present, laparoscopic cholangiography was performed. For this, two 3 mm trocars were placed, one in the right hypochondrium and the other just to the left of the midline midway between the umbilicus and the xiphoid process. Under direct vision provided by the laparoscope, a laparoscopic needle of 16 gauge was inserted into the gall bladder through the trocar placed in the right hypochondrium. Diatrizoate meglumine contrast was injected through the needle into the gall bladder to opacify the proximal and distal biliary tree and serial X-rays taken. A piece of liver tissue from the lower edge was taken for histopathological examination. Hemostasis was performed using a monopolar electrocautery. The decision of the surgical procedure was made according to the results obtained with the laparoscopic exploration and laparoscopic cholangio-graphy. If the passage of dye into the proximal and distal biliary tract was seen, the procedure ended with the liver biopsy and diagnosis of neonatal hepatitis was made. If the gall bladder was found to be atretic, or no passage of dye into the biliary tract was seen (Fig. 1), the diagnosis of EHBA was made, and Kasai’s portoenterostomy was performed. The patients were monitored peroperatively with pulse oximetry, capnography, non-invasive blood pressure, continuous temperature monitoring and precordial stethoscope. Results From February to September 2001, six patients, four boys and two girls with conjugated hyperbilirubinemia were evaluated laparoscopically. Their age ranged from two to four months. Free passage of dye into the proximal and distal biliary tree was noted in three patients whereas no passage of dye with an atretic gall bladder was noted in the rest. Kasai’s portoenterostomy was performed in all these patients. Hence laparotomy was avoided in three patients. No complication associated with the laparoscopic procedure was recorded. The mean operating time for the laparoscopic procedure was 30 to 35 minutes. Liver biopsy taken at the time of laparoscopy confirmed the findings of laparoscopy and cholangiography. Discussion During the evaluation of an infant with prolonged jaundice, besides the biochemical and serologic tests, abdominal ultrasono-graphy, hepatobiliary scintigraphy and fine needle or trucut liver biopsy is carried out(1-3). The positive "triangular cord sign" in the abdominal ultrasonography is highly sugges-tive of EHBA(4). In the present study, ultrasound was done in all the cases. However, it was suggestive of EHBA in only two cases. The gall bladder could not be visualized in the remaining four cases. A percutaneous liver biopsy was done in all the patients before they were referred to us. All results were suggstive of EHBA. Needle biopsy in biliary atresia shows proliferating bile ducts whereas in neonatal hepatitis, giant cells and focal areas of necrosis are suggestive. Although liver biopsy appears to be the definitive diagnostic test in differentiation between biliary atresia and neonatal hepatitis indicating laparotomy in previous days, there are many instances where the biopsy reports are equivocal. There is a considerable overlap of atresia patients often having occasional giant cells(3-5). If it is performed before four to eight weeks of age in infants who have biliary atresia, it may not show the characteristic ductal proliferation or portal fibrosis necessitating a second biopsy as shown in the work by Park et al.(6). False postive results can occur in cholestatic liver diseases such as bile plug syndrome, alpha-1 antitrypsin deficiency and in some cases of neonatal hepatitis(3,5,7). Hepatobiliary scintigraphy using Tc-labeled agents is widely used for differentiation between EHBA and other causes of infantile cholestasis. Apart from the disadvantages of low specificity (i.e. false positive scans as high as 25%-30%) and radiation safety hazards, priming of the patients 2-3 days before tests is necesary to reduce the false positive results. Over and above all these, it dose not provide histological diagnosis. In addition to this, isotope scans also show an absence of hepatic excretion in conditions like insppissated bile syndrome and interlobular biliary hypoplasia, which cannot be differentiated from EHBA without the help of liver biopsy. The study performed by Spivak et al.(8) showed that infants with low birth weight less than 2200 g, premature infants, infants on total parenteral nutrition and infants with severe neonatal hepatitis are prone to have no gut excretion of tracer. In the present study, because of economic restraints and lack of availability, HIDA scan was done in two patients which was suggestive of extra hepatic biliary atresia. However, on cholangiography, one of the two children had a patent extra hepatic biliary tree. Thus, the sensitivity in the present study was 50%.
Laparoscopy as in many other areas has found a great spectrum of indications in pediatric surgery. Before the introduction of laparoscopy, laparotomy had to be performed on the infants with prolonged jaundice in whom neonatal hepatitis could not be differentiated with laboratory, radiologic and histopathologic investigations. Laparotomy with or without cholangiography, although an effective method in differentiation, brings unnecessary risks to the infants with neonatal hepatisis and complications like wound dehiscence and evisceration of the bowel are common. The larger the wound, the more are the muscles and nerves stretched or cut, and thus more pain or restriction of movements is expected postoperatively. Large wounds would also lead to big scars. Even if open surgery is performed through small incisions, the amount of stretching that would be required to expose the organ properly, would many a times lead to postoperative problems. On the other hand, laparoscopy and laparoscopic cholangiography has helped to distinguish between biliary atresia and giant cell hepatitis with 96% accuracy without causing any harm or damage(9). CO2 insufflation above 15 mm Hg in pediatric patients can cause compression of the inferior venacava and a decrease in venous return and hypotension. A pressure of more than 6-8 mm of Hg in newborns can cause reopening of th left-right shunts and in turn cause hypoxemia. We had maintained a CO2 pneumoperitoneum between 6-8 mm of Hg during the entire procedure. Non-invasive blood pressure monitoring and capnography also guided us to control the CO2 flow and pressure. If the CO2 levels rose above 35, the CO2 pressure was temporarily reduced till the levels normalized. This hardly took a minute. Laparoscopic examination of the liver with simultaneous cholangiography is a simple procedure that provides a chance to achieve an earlier and accurate diagnosis for neontal jaundice(1). This approach, after abdominal ultrasonography could be performed as the second step of the diagnostic evaluation in neonates with prolonged jaundice. Diagnostic laparoscopy is a direct method to visualize the liver and gall bladder and when it is combined with the cholangiographic examination, the important period of time for the surgical success in EHBA, will be minimally wasted. This procedure because of its simplicity should be considered as a diagnostic modality which could assist pediatricians to evaluate children with jaundice and save a lot of time searching for nonsurgical causes thinking that they may save the child from surgery. Contributors: AVS co-ordinated the study and drafted the paper. He will act as guarantor for the manuscript. AAS participated in the data collection, and drafting the paper. AMS particiapted in data collection. Funding: None. Competing interests: None stated.
| ||
|
References | ||
|
![]()