|
|
Brief Reports Indian Pediatrics 2002; 39:1131-1137 |
||
|
Thoracoscopic Thymectomy for Juvenile Myasthenia Gravis |
||
|
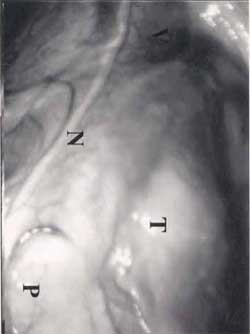
Myasthenia gravis (MG) is an autoimmune disorder characterized by antibody-mediated damage to the acetylcholine receptors at the neuromuscular junction of the skeletal muscles. It results in muscular weakness, which is most profound on fatigable stimulation. In the absence of a clearly identified etiology, the treatment has been largely symptomatic and consists of anticholinesterase drugs (neostigmine/pyridostigmine), immune-modifying agents (steroids, intravenous immunoglobulins and cytotoxic drugs), and plasmapheresis. Complete thymectomy has been shown to relieve symptoms and induce remission in many patients (adults as well as children)(1). While thymectomy is a well-accepted and widely used treatment option in adult MG, its full potential has not been realized in the treatment of juvenile MG due to ignorance about the benefits of thymectomy in children and fears of possible ill effects of thymectomy at young age. Morbidity and cosmetic problems associated with "sternotomy", which was hitherto required to perform thymectomy is another major reason. With the introduction of video-assisted-thoracoscopic techniques, it is now possible to perform complete thymectomy without the need for sternotomy(2,3). This report describes our experience with thoracoscopic thymectomy in 9 adolescents with myasthenia gravis. Subjects and Methods At the All India Institute of Medical Sciences, New Delhi, 32 patients of generalized MG underwent thoracoscopic thymectomy between October 2000 and February 2002. Out of them, 9 were adolescents (age <18 years) qualifying to be called Juvenile MG. These subjects form the basis of this report. Their records were analyzed to study the demographic data, the age at presentation, stage of MG at presentation, initial medical treatment provided, time gap between the diagnosis and thymectomy, the approach used for performing thymectomy, operating time, intraoperative and postoperative complica-tions (including blood loss and need for transfusion), duration of ICU stay, chest tube duration and postoperative hopsital stay. Results The demographic and other details of these 9 patients are provided in Table I. Their age ranged from 4-18 years (mean 14.3 years). The duration of illness before surgery ranged from 2 months to 84 months. The clinical stage was mostly IIa. The diagnosis of myasthenia gravis in these patients was based on clinical features complimented by positive tensilon test or repetitive nerve stimulation test. Anti-acetylcholine receptor antibodies were tested in only 3 patients and were positive. None of the patients had clinical or biochemical evidence of thyroid dysfunction. Except one patient, all of them were on pyridostigmine (90-180 mg/day). Three patients were on steroids in addition to pyridostigmine. One patient had past history of receiving steroids for 3 months, 8 months back. None had required cytotoxic drugs or plasmapheresis. Only one patient had associated autoimmune disease in the form of juvenile rheumatoid arthritis. One patient (case no. 6) had history of myasthenic crisis 6 months back requiring ventilatory support for two months. The procedure was performed under general anesthesia with double lumen endotracheal intubation to achieve single lung ventilation during surgery. A combined cervical and right thoracoscopic approach was used in 6 patients and a combination of cervical and bilateral thoracoscopic approach in remaining 3 patients. The entire mediastinum from the thoracic inlet to the diaphragm was clearly visible and explored easily. All the major nerves and vessels were clearly visualized (Fig 1). Whole of the thymus gland along with the mediastinal fat was removed. The operating time ranged from 120-360 minutes (mean 206 minutes). The blood loss was minimal and none of the patients needed transfusion. There were no intra-operative complications. Complete thymectomy could be performed thoracoscopically in all the patients. No patient required conversion to thoracotomy. All were extubated on the operating table and transferred to the intensive care unit (ICU) for monitoring and observation. All the patients were allowed orally the same evening and next morning, they were shifted to the surgical ward after removal of the chest tube. Post operative pain relief was provided by morphine infusion of 10 µg/kg/hour or intramuscular diclofenac sodium 8 hourly for the first 18-24 hours. As soon as the patients had taken orally, oral painkillers were started. This regimen provided adequate pain relief. Epidural catheter for analgesia was not required in any patient. There were no postoperative complications in any patient. Oral medications for MG were restarted on postoperative day one in all the patients in same pre-operative dosages and they were discharged from the surgical ward on 2nd or 3rd postoperative day. During a mean follow up of 10 months (range 1 to 16 months), there was reduction in the drug requirement in all patients with symptomatic improvement. However, due to the short follow-up, none of the patients is yet in complete remission. Discussion Thymectomy is a well-accepted treatment for autoimmune myasthenia gravis. Among currently available treatment modalities, it is the only one that offers a chance of "cure" (complete remission with no need for further therapy) in some patients. In adults, the benefits of thymectomy are well established and it is a well accepted part of the treatment algorithm of these patients(4). Numerous studies have demonstrated consistently higher remission rates following thymectomy compared to medical treatment in children also(1,5-10). The degree of benefit accruing from thymectomy relative to spontaneous remission has however, varied widely from as low as 10-23% to as high as 57% in a subset of patients(6,8). The factors responsible for such variation in children are age of the patient, timing of surgery and racial factors. Lakhoo et al.(11) reported a strong association between young age and early surgery with better outcome. In their series of 15 black children, all were pre-pubertal and thymectomy was performed within 3 months of diagnosis in 75% of them. On follow up, 83% children were on minimal medication or in total remission. Racial factors are also important and according to Andrews et al(7), white children do better than black children following thymectomy. Timing of surgery is another crucial factor, with consistently higher remission rates reported when surgery was performed within 1-2 years of diagnosis (1,6,8,11). Some authors have suggested delaying thymectomy till puberty fearing ill effects of early thymectomy on development of the immune system in early life(12,13). However, on critical analysis of early-thymectomized children, no clinical problems have been reported on long-term followup(1). It has also been reported that children with hyperplastic glands show better prognosis than those with histologically normal gland(1)). Unfortunately, despite this knowledge, many institutions continue to keep the children on medical therapy, reserving thymectomy for those with very severe symptoms or those not responding to medical therapy(14,15). The reasons for this reservation are not far to seek. Fears about the possible ill effects of early thymectomy and morbidity associated with sternotomy, which is required to perform thymectomy, are the two main reasons. Fears of post thymectomy sepsis and post thymectomy neoplasms have been proved to be unfounded on close scrutiny and long term follow up of the early-thymectomized children(1). However, sternotomy related problems continue to bother physicians as well as patients. The wound pain, chest infection, prolonged hospital stay and an unsightly long scar at the prominent place are the main problems associated with sternotomy.
Video-assisted-thoracoscopic-surgery (VATS) offers the possibility of performing "complete" thymectomy in a minimally invasive manner(16). As the thymus is a midline structure, it can be approached from either the right or the left side. Accordingly there is a right thoracoscopic approach, a left thoracoscopic approach and a bilateral thoracoscopic approach. The thymectomy can be carried out successfully through either of these approaches(17,18). At the end of the procedure, a chest tube is left to drain the pleural cavity, which is usually removed at 24 hours and patients can be discharged in 2-3 days time. Novellino et al.(19) reported the first series of thoracoscopic thymectomy in adults in 1994. Since then, numerous reports in the literature have testified to the safety and adequacy of thoracoscopic thymectomy in adults(16-21). Although the mean operating time has been reported to be the same as that in open surgery, the postopeative pain is much reduced with reduced postoperative analgesic requirements. Furthermore, the hospital stay is shorter thereby reducing the overall hospitalization costs and return to studies/work is quicker. The cosmetic results after thoracoscopic thymectomy are far superior. In the intermediate term follow up results reported in numerous series till now, the remission rates have been same as those achieved with open thymectomy(16,18,20). Thus, thoracoscopy is emerging as an equally effective, minimally invasive alternative to conventional sternotomy for the performance of thymectomy in patients with MG. Kolski et al.(3) compared 6 children who underwent thoracoscopic thymectomy with 6 other children who had undergone transsternal thymectomy. The age of the children in the thoracoscopy group ranged from 1.6 to 14.6 years (mean -10.5 yr). The operating time and the cost of the procedure were same in both the groups. However, the postoperative hospital stay was significantly shorter in VATS group, and hence, the overall cost of the procedure was significantly reduced (P <0.05). Cosmetic appearance was far superior in the VATS group. In a mean follow up of 2.7 years, all the 6 patients in the VATS group showed same improvement as in the sternotomy group. Kogut et al.(2) reported their experience with VATS thymectomy in 10 children(2). The mean operating time was 114 minutes. There were no intra-operative or post-operative complications. All except one patient were discharged on the morning of the first post-operative day. One child with pre-operative respiratory weakness was discharged on post-operative day 3. They concluded that VATS thymectomy could be safely done in children. Compared to the scar resulting after sternotomy, the cosmetic advantage of VATS approach is obvious (Fig. 2). Based on the literature review and our own experience, we believe that thoracoscopic thymectomy can be performed safely in children. It should be offered to children with generalized MG as early in the course of their disease as possible, preferably within the first year. This approach will offer these children best chance of long term remission with all the benefits of minimally invasive surgery. Contributors: All the authors were involved in care of the patients and drafting of the manuscript. The operations were done by a team consisting of AK, SK, and RG. DKP was the anesthetist and SS and VK followed up the children following surgery. AK shall act as guarantor of the study. Funding: None. Competing interests: None stated.
| ||
|
References | ||
|
![]()