|
|
Case Reports Indian Pediatrics 2001; 38: 1419-1421 |
||
|
Goldenhar Syndrome with Congenital Athyrosis |
||
|
V.V. Khadilkar A.V. Khadilkar
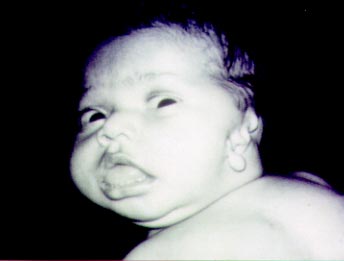
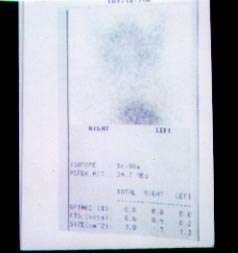
Goldenhar syndrome was first described by Von Arlt in 1845, however it was precisely defined by Goldenhar in 1952(1). It usually consists of pre auricular appendages, fistulae, hypoplastic or absent pinnae, anti-mongoloid slant, coloboma of the iris and lids, epibulbar dermoids, macrostomia, microphthalmos, hypoplastic maxilla and mandible, cleft palate, hemi-vertebrae and other vertebral anomalies. In the recent times association of cardiac defects, lung defect, CNS defects, renal anomalies and limb deformities have been described. We report for the first time an association of congenital athyrosis with Goldenhar syndrome. Case Report A 6-month-old female infant, second child of consanguineous marriage presented with history of severe developmental delay, large tongue, constipation and abnormality of the right ear. On clinical examination baby had absent left pinna which was replaced by periauricular skin tags and appendages, atresia of the left external auditory canal, epibulbar dermoid, macrostomia on the left side with hypoplastic mandible. In additon to these features suggestive of Goldenhar syndrome baby had obvious clinical signs of hypothyroidism in the form of large tongue, umbilical hernia, widely open anterior fontanelle, open posterior fontanelle, pallor, constipation, hypotonia, dry thick scaly skin and severe developmental delay (Fig. 1). Her investigations showed a TSH of more than 45 miu/L, T4 0.1 of mcg/dl and T3 of 0.02 ng/ml. The lower femoral epiphysis had not appeared even at 6 months of age. Tc99 thyroid scan was done which failed to demonstrate any thyroid tissue indicating conenital agenesis of thyroid gland (Fig 2). There were no vertebral anomalies in our patient. Brainstem Evoked Response Audio-metry showed normal hearing on the right side and absent I, II, III, IV and delayed V waves suggestive of a peripheral lesion on the left side. Thyroxine replacement therapy was started immediately following the diagnosis. On replacement therapy she made impressive
Discussion Goldenhar syndrome, Treacher-Collin syndrome (MFD) share some common features such as malformed ears, sensori-neural deafness and hypoplasia of the mandible. However, in Goldenhar syndrome the hypoplasia is asymmetrical and presence of epibulbar dermoid is charactersitic. Athyrosis is not reported with Goldenhar syndrome earlier and we report it for the first time. Goldenhar syndrome is a defect of the structure arising from first and second branchial arches, the first branchial pouch, the first branchial cleft and the primordia of the temporal bone. In a recent report(2), polydactyly and hydrocephalus have been described as associations of Goldenhar syndrome. The thyroid gland originates as an epithelial proliferation in the floor of the pharynx at the point of foramen caecum which is at the junction of the anterior two thirds and posterior one third of the tongue. The anterior two third of the tongue originates from the first branchial arch while the posterior one third originates from the 2, 3 and 4 branchial arches(3). As Goldenhar syndrome is a malformation sequence of these branchial arches and pouches, embyro-logically it makes sense that Goldenhar syndrome may be associated with thyroid agenesis and hence thyroid agenesis could be a part of the same sequence that leads to Goldenhar syndrome. In our extensive search of published data we failed to find reports of this association with Goldenhar syndrome. Congenital hypothyroidism is a condition in which the mental retardation is potentially preventable when diagnosed early and treated effectively. Embryologically there could be a higher chance of having hypothyroidism in children with defects of first and second branchial arches and pouches. It may be therefore prudent to screen neonates with defects of the first and second branchial arches and pouches such as in Godenhar syndrome and Treacher Collin syndrome with thyroid function tests so that mental retardation can be prevented. Contributors: Both authors were involved in the care of the patient and drafting the manuscript. VVK will act as the guarantor for the paper. Funding: None. Competing interests: None declared.
| ||
| References | ||
|
![]()