|
|
Technology Update Indian Pediatrics 2001; 38: 1382-1392 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
The clinical application of bronchoscopy dates back to 1897 when Killian removed a pork bone from the right main bronchus in a farmer. Flexible fibreoptic bronchoscope was introduced in 1967 by Dr. Shigeto Ikeda(1). Due to technical limitations its use was initially restricted to adults. With advances in technology it has been possible to reduce the size of the fibreoptic bronchoscope thus allowing its use in infants and children. The use of flexible bronchoscopy in children has expanded from assisting visual diagnosis to include diagnostic procedures such as bronchoalveolar lavage (BAL) and trans-bronchial biopsy (TBB). The relatively large internal diameter of the rigid bronchoscope allows the use of auxiliary equipment (grasping devices, baskets, forceps) and hence is preferred for removal of foreign bodies. The posterior commissure of the larynx is better visualized with the rigid bronchoscope as it approaches the larynx from an anterior angle. Flexible bronchoscopy has also found a useful role in the intensive care unit and in assisting endotracheal intubations. The advantages and disadvantages of flexible and rigid broncho-scopy are presented in Table I. The last decade has seen tremendous progress in adult interventional bronchoscopy and the progress in the pediatric age group is also encouraging(2,3). Equipment and Instrument Selection The different parts of the flexible broncho-scope are: (i) the eye piece; (ii) angulation control lever; (iii) angulation lock; (iv) working channel; (v) suction connector; (vi) insertion tube: at the distal end has objective lens, light guides and instrument channel (which is also the suction channel) and has a bending section at the tip of the endoscope; and (vii) universal cord which connects to the light guide connector section. The various sizes of flexible broncho-scopes (representing outer diameter) commonly available for pediatric flexible bronchoscope (PFB) range from 2.2 mm to 4.9 mm (Table II). We use a special camera to attach the bronchoscope to a video system, which allows an enhanced image to be viewed on a monitor while performing the procedures. We also perform video recording of most procedures, as they are useful for archiving purposes and also allow discussion of the findings with the family and the referring doctor. Bronchoscopes that are 3.2 mm or more in diameter usually have a working channel, which facilitates suction and also allows passage of biopsy forceps. Bronchoscopes that are 2.2 mm or less in diameter (do not have a working channel) are particularly useful in the intensive care unit and are also used in neonates. These endoscopes are also useful in assessing nasal space and laryngeal/vocal cord pathology. Table I__Flexible v/s Rigid Bronchoscopy
Anesthesia PFB can be performed both under general anesthesia as well as local anesthesia. In Australia, currently gaseous inhalation general anesthetic technique is used in most centers (personal communication). However, many centers around the world have a pre-ference for sedation and local anesthesia(2,4). Our experience with the use of general anesthesia has been favorable as the patient is more settled and allows easy passage of the bronchoscope, especially in the younger age group. Having an anesthetist is an advantage for patient monitoring, control of the airway and an extra assessment of potential risk. The disadvantages of this approach are the potential irritant effect of the anesthetic gas on the airways and the additional theatre costs. General Anesthesia At our institute gaseous induction is usually undertaken with halothane, sevo-flurane and oxygen. Local anesthesia (1% or 2% lignocaine) is applied directly to the larynx and trachea via a Cass needle. Intravenous induction with agents such as propofol with subsequent gaseous anesthetic maintenance is often used in the older children. The bronchoscope is passed through a swivel, which connects to a facemask or a laryngeal mask or an endotracheal tube. In our experience the laryngeal mask has a useful role to control ventilation especially when the indication of bronchoscopy is to perform a bronchoalveolar lavage and the upper airway may not be visualized. Most elective procedures are performed in a day surgery setting with 2 hours post-operative observation. Sedation and Local Anesthesia The goals of sedation are to allow the patient to remain comfortable while main-taining adequate ventilation and oxygenation despite the use of bronchoscope in the airway. The medications commonly used for sedation are fentanyl 1-3 mcg/kg/h and midazolam 0.1 mg/kg(5,6). Reversal agents (naloxone and flumazenil) may be used in the post-operative period. In adult patients who undergo flexible bronchoscopy under local anesthesia and sedation (St. Vincent’s Hospital, Sydney) the commonest indication for use of reversal agents is for patients who develop respiratory depression. Topical lignocaine in doses up to 8 mg/kg can be used safely(7). Lignocaine jelly (2%) is applied to the nostril and 2% lignocaine is sprayed on the cords, trachea and bronchial tree through the working channel of the bronchoscope as required. Anatomy for the Bronchoscopist We introduce the bronchoscope through the nostril or the endotracheal tube in intubated patients. With the patient in the supine position, and the bronchoscopist at the head end of the patient, the palate will appear at the top, and the posterior pharyngeal wall and the adenoids at the bottom. Beyond the edge of the soft palate, the larynx, esophagus, and the base of the tongue are visualzed. We evaluate the dynamics of movements of the larynx after the examination of the tracheobronchial tree. The bronchoscope is placed just above the larynx and movements are evaluated as the child is made to wake up from general anesthesia. When preformed under local anesthesia, these are usually observed before traversing the vocal cords. There are considerable differences between the infant and the adult larynx. The infant larynx is placed more anteriorly in the neck compared to the adult, and it often appears to stand up on a pedestal from the floor of the pharynx. The epiglottis has a much more pronounced curvature (omega or U shaped) compared to the adult epiglottis and the arytenoid cartilages may be very prominent in the infant. In contrast to the adult, the cuneiform and corniculate cartilages may not be discernible as separate structures in the child. The sub glottic space is the narrow portion of the airway in infants and young children as compared to the glottis in the adults. Hence, the selection of bronchoscope for infants and young children should take into consideration that the area beneath the vocal cords is the area of limitation, not the space between the vocal cords as in adults(6). The trachea is entered after passing the cricoid cartilage. In children the trachea is nearly round, with the cartilages extending visibly through an arc of approximately 320 degrees. It is normal to see some inward protrusion of the membranous portion of the airways (trachea and main bronchi) on coughing. The main carina is keel shaped and oriented in an anteroposterior plain. In the adult the main carina is sharp and a widened carina in adults may indicate subcarinal lymphadenopathy. In the child the main carina is often quite blunted. The right mainstem bronchus is immediately seen on peering down the trachea. The left main bronchus can be visualized in its entirety from the carina, after turning towards the left, and even then it takes a curving course so that its bifurcation cannot be seen from the carina. The shape of the main stem bronchi is very similar to that of the trachea, with a prominent posterior membranous portion. The right upper lobe division takes off just beyond the carina at an angle of approximately 100 degrees. The right upper lobe bronchus itself may have a length of 1cm before dividing into the anterior, posterior and apical segmental bronchi. Beyond the origin of the right upper lobe bronchus, the right main stem bronchus continues as the bronchus intermedius. This bronchus may extend for 2-2.5 cm at which point it gives rise to the middle lobe bronchus anteriorly, the superior segment of the right lower lobe posteriorly and the right lower lobe bronchus that divides into basilar segments. The left mainstem bronchus is 4-4.5 cm in length and terminates into the upper lobe and lower lobe bronchi. As the left upper lobe bronchus ascends superiorly, the lingular bronchus arises and extends slightly down-ward in an inferior-lateral direction. The upper division bronchus of the upper lobe passes beyond the orifice of the lingula and gives rise to the apicoposterior and the anterior segments. Immediately on entering the left lower lobe bronchus arises the superior segment of the left lower lobe and that descends posteriorly. The left lower lobe bronchus beyond the origin of the superior segment is usually 1 cm in length before giving rise to the basal bronchi. Indications The indications (Table III) for diagnostic bronchoscopy are both symptom and diag-nosis driven. The common indications for PFB in our hospital are stridor, persistent cough, persistent opacity on the chest radio-graph, and investigation of the immuno-compromised child. As reported, stridor forms one of the most common indications for bronchoscopy in children(8). It is indicated when the symptoms are severe or persistent or when there is a doubt regarding the diagnosis. It may also be considered if stridor worries the parents or the treating physician. The common causes of stridor are laryngomalacia or tracheomalacia, vocal cord paresis, sub glottic cysts or stenosis and extrinsic compression of the trachea (vascular ring or innominate artery compression). Persistent cough can be a very frustrating symptom to evaluate and treat. If reactive airway disease and psychogenic causes can be excluded, flexible broncho-scopy may reveal unsuspected foreign bodies, tracheomalacia, bronchomalacia, extrinsic compression in the tracheobronchial tree or gastro-esophageal reflux(9). Unilateral or a localized wheeze is a definite indication for bronchoscopy. In case of bilateral wheezing, bronchoscopy is indicated if it were persistent or poorly responsive to optimal broncho-dilator therapy(10). The common findings in these situations are unsuspected foreign bodies, tracheomalacia, bronchomalacia or airway stenosis. Table III__Indications for Flexible Bronchoscopy
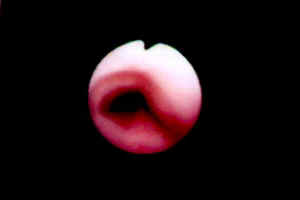
Persistent crackles in a localized area and recurrent or persistent infiltrates on the radiograph also form common indications. In these situations bronchoscopy is performed to obtain a lavage specimen (particularly if an adequate sputum sample cannot be obtained), to rule out the presence of a foreign body and therapeutic suction in case of mucous plugging. Bronchoalveolar lavage (BAL) is a safe and sensitive technique for investigating infectious causes of respiratory disease. In the immunocompromized child BAL is used to obtain samples for microbiology and cytology studies(2). Our referral for this group of patients is mainly from the hematology-oncology unit. Quantitative bacterial cultures of BAL have been used to diagnose pneumonia in immunocompromized and immunocompetent patients. When BAL with <1% squamous epithelial cells was analyzed, the finding of >105 colony-forming units of a single bacterial species per ml of BAL was correlated with bacterial pneumonia in comparison with normal subjects(11-13). In immunosuppressed patients with diffuse lung infiltrates, P. carinii can be identified in BAL with a sensitivity of up to 85%(14-17). Based on response to therapy or histology findings on biopsy or autopsy, the absence of P. carinii in BAL in immunosuppressed patients has a negative predictive value of >90%(16-18). In these patients, the sensitivity for detecting M. tuberculosis is up to 95%. The negative predictive value of absence of M. tuberculosis on BAL is > 90%(16,17). The role of BAL in monitoring interstitial diseases and chronic infective disorders such as tuberculosis and cystic fibrosis is controversial and undefined for routine use(19-22). The small size of the working channel is one of the limiting factors for performing a TBB through the pediatric flexible bronchoscope. The dominant role of TBB is in interstitial lung disease and immunocompromized individuals including lung transplant recipients(2,23). Some illustrative photographs of clinical conditions encountered by us are depicted in Figs. 1-9. Interventional Bronchoscopy Both flexible and rigid bronchoscopy have a role in the management of foreign bodies in the tracheobronchial tree. The larger working channel in the rigid bronchoscope allows better instrumentation for foreign body removal and is the instrument of choice in these situations. When there are obvious reasons (asphyxia, radiopaque foreign body or association of unilaterally decreased breath sounds and obstructive emphysema) to believe aspiration of a foreign body, rigid bronchoscopy should be the procedure of choice. When there is a doubt regarding the aspiration of a foreign body, flexible bronchoscopy provides a simple and safe method to confirm its presence(24). In these situations the flexible approach is preferable, as the procedure is quicker, less traumatic than rigid instrumentation and also allows detailed examination of distal airways. In the Lung Transplant Unit at St. Vincent’s Hospital, we employ balloon dilatation techniques, placement of tracheobronchial prosthesis and Nd-YAG laser for management of various benign and malignant lesions in adult patients. The experience with these interventions in the pediatric population is limited. However, preliminary experience with the use of balloon dilatation(2) and expandable metallic airway stents for tracheobronchial stenosis in the pediatric population is encouraging(3).
Flexible bronchoscopy can be used safely to assess the position and patency of endotracheal tubes. In the assessment of endotracheal tube position it is as effective as radiological assessment and at the same time avoids exposure to radiation(25-27). Premature infants may develop mucous plugs or endobronchial granulation tissue as a result of trauma from an endotracheal tube or suction catheters. We use ultrathin flexible bronchoscopes via an endotracheal tube to evaluate the airways in both premature and newborn infants. Concerns regarding the state of the airways often arise in a child with a tracheostomy. In these cases, the trachea may be examined for the presence of granulation tissue or stenosis at the site of tracheostomy. Retrograde laryngoscopy may be performed through the tracheostomy stoma to evaluate the sub glottic area and the larynx. Flexible bronchoscopy is an invaluable tool in accomplishing endotracheal intubations in the operation theatre as well as in the intensive care unit for patients with a difficult airway(2). It may provide useful diagnostic information as to the cause leading to the difficulty. Flexible bronchoscopy may also be used in defining tracheoesophageal fistula and to guide the extent to surgical manipulations intraoperatively for aortopexy/tracheopexy procedures. These are uncommonly used skills for a bronchoscopist but require high level of training and skills that usually evolve with an experienced bronchoscopist. Role in Pulmonary Tuberculosis PFB allows the demonstration of endo-bronchial tuberculous lesions and permits collection of specimens for mycobacterial studies. Demonstration of endobronchial lesions and/or extrinsic compression (lymph nodes) occluding more than 50% of main stem bronchi, is a useful guide to initiate prednisolone therapy(28). The bacteriologic yield for mycobacteria has been shown to be better with gastric lavage comparing bronchoalveolar lavage(29). However, we feel that BAL has an important role in situations when there is strong clinical suspicion and other methods to isolate mycobacteria have failed. The isolation of the mycobacteria is useful for antibiotic sensitivity testing especially where multiple resistant M. tuberculosis strains are prevalent as well as for epidemiological purposes. Bronchoalveolar Lavage Bronchoalveolar lavage allows the recovery of both cellular and noncellular components from the epithelial surface of the lower respiratory tract and differs from bronchial washings, which refer to aspiration of either secretions or small amounts of instilled saline from the large airway(30). When the lung pathology is a diffuse process, BAL is performed from the lingula and the right middle lobe because of their favourable anatomical location, ease of obtaining a good wedge, and a higher volume of returning fluid as compared to the other lobes(31). When the pathology is localized, BAL is obtained from the affected segment. Various methods have been used to estimate the maximum volume of BAL fluid that can be used safely in young patients. In children over 3 kg of weight, 1 to 3 aliquotes of 5-10 ml each are used upto a maximum of 3 ml/kg(8). Some centers restrict the amount of lavage fluid to no more than 5-15% of the functional residual capacity (FRC). The FRC may be measured by spirometry or estimated from the patients height using the following equation: FRC = 1.3 to 1.5 ml × height or length in centimeters(9). To perform a BAL, the bronchoscope is advanced to the selected segment until it can go no further with gentle pressure (wedge position). Sterile normal saline is then instilled via the suction port in 5-10 ml aliquot’s and fluid is then recovered into a specimen trap in-line to the wall suction. Manual suction with a syringe may also be used to recover the lavage fluid(6). Contraindications Flexible bronchoscopy is a safe and well-tolerated procedure. Premature age and size (weights <800 g) are generally not contra-indications as instruments are now available to deal with these size factors. Patients with massive hemoptysis, severe airflow obstruc-tion, severe refractory hypoxemia, and unstable hemodynamics including dysarhyth-mias present a serious risk of complica-tion(32). Flexible bronchoscopy or laryngo-scopy is not indicated in acute stridor as it may lead to the progress of a partial obstruction to a total obstruction. The common causes of acute stridor are croup, epiglottitis or a laryngeal foreign body. Complications Epistaxis is a mechanical complication associated with the nasal insertion of the bronchoscope and is seen more often with the learning bronchoscopist. It is important not to force the bronchoscope through the nostril. Its passage should be smooth and under vision. If there is difficulty in passing through one nostril the other one should be tried. On rare occasions it may not be possible to pass the bronchoscope through either nostril and in these circumstances one may choose to pass it through the oral cavity. Topical epinephrine may be used in cases of significant bleeding. In case of epistaxis blood may trickle down to the larynx and sometimes into the tracheo-bronchial tree. This can pose difficulties if the purpose of the procedure was to identify the site of bleeding in a patient with hemoptysis. The important causes of hypoxemia during bronchoscopy are increase in airway resis-tance, excessive sedation and disturbances of the ventilation perfusion relationship(32). Tachycardia may be the first sign of impending hypoxia. Bradycardia is always a signal for the bronchoscopist to immediately remove the bronchoscope from the airway and to support ventilation. For patients with re-active airway disease, mechanical stimulation of the airways may result in bronchospasm. This usually responds well to nebulized salbutamol given soon after the procedure. If the tip of the bronchoscope is left wedged into a bronchus while the patient coughs, the mucosa can be torn and on the rare occasion a pneumothorax or a pneumomediastinum may result. Pneumothorax may also occur following a transbronchial biopsy. Post bronchoscopy fever lasting up to 24 to 48 hours is usually transient and almost always self-limiting and is seen more commonly after a bronchoscopic lavage. In a series of 1095 procedures the overall incidence of complications was 2.9%, which included transient bradycardia (1%), epistaxis (0.7%), laryngospasm (0.3%), anesthetic complica-tions (0.5%), and pneumothorax (0.2%)(8). When performed under local anesthesia, excessive use of sedation may lead to respiratory depression. Inadequate use of topical anesthesia can result in bradycardia and laryngospasm(32). Instrument Cleansing and Storage In all cleaning processes, toilet/flushing/brushing of the suction port immediately post bronchoscopy while the secretions are still moist is very important to prevent potential obstruction of the endoscope. We use peracetic acid, a low temperature and chemical cleansing/sterilizing agent with non-toxic residuals when used in equipment such as Steris System (Steris Corporation Mentor, USA). High level of disinfection, defined as a procedure that inactivates all fungi, viruses, and vegetative micro-organisms, but not necessarily all bacterial spores, can be achieved with 2% glutaraldehyde(33). Immer-sion in glutaraldehyde for 10 minutes will destroy bacteria, viruses, and 99.8% of myco-bacterial organisms. Immersion in glutar-aldehyde for 45 minutes at 25ºC will destroy all mycobacterial organisms. Bronchoscopes are stored best by hanging and the storage cases should be used only for transport purposes. Contributors: PNC designed and drafted the article. PC supervised and helped in the drafting of the article and will act as the guarantor for the paper. Funding: None. Competing interests: None stated.
References
|
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()