|
Personal Practice Indian Pediatrics 1999;36: 1229-1242 |
||||||||||||||||||||||||||||
Current Trends in Management of the Beta Thalassemias |
||||||||||||||||||||||||||||
| Dheeraj Shah, Panna Choudhury, A.P.
Dubey From the Department of Pediatrics,
Maulana Azad Medical College and Associated Lok Nayak Hospital, New Delhi 110 002, India. |
||||||||||||||||||||||||||||
|
Thalassemia syndromes are a heterogenous group of disorders resulting from the inability of the patients' red cells to synthesize an adequate amount of either the alpha or the beta chains in the hemoglobin molecule. Accordingly the condition is broadly divided into alpha or beta thalassemia. The beta thalassemias have emerged as a huge public health problem worldwide(1). Increase in survival of patients with these disorders represents one of the most dramatic alterations in morbidity and mortality associated with a genetic disease in this century and the subject is being constantly reviewed(2). In India, it is estimated that nearly 8,000-10,000 new thalassemics (homozygous) are born every year and the beta thalassemia gene is more commonly found in Punjabis, Sindhis, Bengalis and Gujaratis(3). Thalassemia intermedia is a genetically heterogenous disease and can result from many different genetic lesions. In eastern India, thalassemia intermedia is mainly due to double heterozygous state of Hb E-beta thalassemia. The clinical expression of beta thalassemia major commences at several months of age, when the waning synthesis of Hb F is normally offset by rising production of Hb A. Marked expansion of the bone marrow takes place as a result of futile attempts to compensate for the worsening anemia resulting from premature destruction of damaged red cells. Children commonly present with anemia and failure to thrive in later half of the first year and in untreated children, characteristic bony changes ensue, including maxillary hypertrophy, frontal bossing and thinning of cortices of long bones predisposing to pathological fractures. Hepato-splenomegaly occurs and rarely high rates of hemolysis lead to jaundice and cholelithiasis. In some patients paravertebral mass have developed that were mistaken for tumors. Ultimately, congestive heart failure ensues and 80% of untreated patients die by the end of second year of life. It is important to differentiate thalassemia intermedia from thalassemia major to plan the transfusion regimen in thalassemia major without delay. This also helps in avoiding unnecessary transfusions and associated complications in thalassemia intermedia. The clinical, molecular and genetic criteria that are used for this differentiation are summarized in Table I(4,5). Thalassemia traits are apparently healthy and normal and are detected usually on a laboratory-screening test. Table I__Criteria for Diagnosis of Beta-Thalassemia Intermedia
The conventional management of thalas-semia is based on a program of regular blood transfusion and iron chelation. This treatment modality itself has seen a progressive transformation of thalassemia major from an invariably fatal disease into a chronic disease permitting a normal life or at least very prolonged survival(6,7). Today the problem of physical appearance has been overcome with regular transfusions and effective chelation therapy. In fact many patients are now getting married and successful pregnancies are being reported all over the world including from India(8). Continuous diligent treatment is the key to the management of thalassemia. Marrow transplantation and gene replacement therapy are the alternatives, which have the possibility of cure. Pharmacological methods to increase gamma chain production, leading to decrease in the amount of free alpha chain and hence less hemolysis are also being tried. The ensuring sections summarize the recent advances in management of thalassemia syndromes. A. Blood Transfusion Regular transfusions are needed for all thalassemics who cannot maintain Hb above 7 g/dl. The goal of transfusion therapy is to keep the Hemoglobin (Hb) level at a minimal baseline level. Such a regimen (hypertransfusion regimen) is currently universally accepted since maintaining a near normal baseline Hb level suppresses the bone marrow almost completely, thus causing reduction in bone marrow volume. Thus, there is not much additional blood requirement as compared to a patient whose bone marrow is greatly expanded because of chronic hypoxia resulting from infrequent transfusions. Maintenance of normal Hb level prevents chronic hypoxemia, hypervolemia, hypersplenism, and promotes normal physical activity and growth. This also checks excess gastrointestinal iron absorption and iron overload. Transfusion therapy may also be important in some intermedia patients as they suffer from hypoxia, though of a lesser degree. By second or third decade they may develop enormous cosmetic defects and increased bone fragility and pseudotumors due to extra-medullary hemopoiesis leading to spinal cord compression. The current recommendation is to maintain a mean Hb level of 12 g/dl. This can be achieved by not letting the Hb fall below 9.5-10g/dl(4). The average rate of Hb fall is 1g/dl per week. Thus raising the post-transfusion Hb to 14 g/dl will allow a 4 weekly transfusion regime with a mean Hb level of 12 g/dl (Table II). For packed cells to raise the Hb by 1 g/dl the blood volume required is 3 ml/kg. Thus in a monthly regime, 12 ml/kg of packed cell is required which is equivalent to 20 ml/kg of whole blood. In 2 weekly regime smaller amounts will be required for the same result. For convenience, a 3 weekly transfusion regime is mostly practiced with pretransfusion Hb level of 10.5 g/dl and post transfusion Hb level of 13.5 g/dl. If the patient is hypersplenic, more frequent transfusions are required. Similarly caution should be exercised to see that post-transfusion Hb level does not exceed 15.5 g/dl. Higher Hb levels increase blood viscosity, reduce tissue oxygenation and increase the risk of thrombosis. The rate of transfusion should be around 5-7.5 ml/kg/h. However, in patients with cardiac problem or severe anemia, no more than 5 ml/kg should be given at one time and rate of transfusion should not exceed 2 ml/kg/h. Table II__ Pre-transfusion Hb Required to Maintain a Mean Hb Level of 12.0 g/dl in Relation to Transfusion Interval
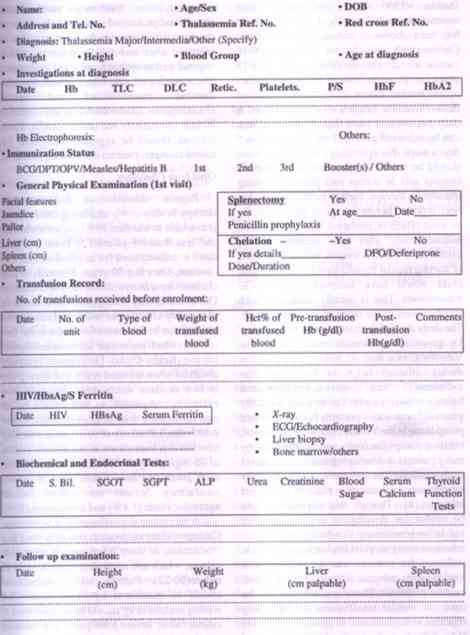
The type of blood to be used for thalassemics is of utmost importance. Blood component therapy has become the order of modern day practice. Thus a thalassemic child should receive group and type specific packed red cells which have been passed through white cell filter(9). This prevents unnecessary infusion of plasma proteins and white cells and thus prevents nonhemolytic febrile transfusion reactions. Filters are also important as these minimize antigenic exposure, which is important because of future prospects of bone marrow tansplantation. Ideally the filters should be used from the outset with each transfusion. However, when resources are limited, use of filters may be limited to only those patients who have recurrent febrile transfusion reactions. Air introduction into the filters can cause major deterioration of function and this is to be avoided. The commonly available filters are Sepacell (Japan), Pall (USA), Leucostop (Italy) and Imugard (Netherlands) and the cost varies from Rs. 600/- to Rs. 1500/- per filter. Care should also be taken to prevent minor red cell incompatibility as well as hemolytic transfusion reactions which may occur due to allo-immunization to minor blood groups. Fortunately majority of thalassemia patients do not develop red cell antibodies and standard cross matching suffices. Prior to transfusion blood should be screened to prevent infections like hepatitis B, hepatitis C, HIV, malaria, syphilis, cytomegalovirus, etc. In fact hepatitis B vaccination is now a routine and must for all HbsAg negative thalassemics. However hepatitis C screening is still not mandatory in India. Evaluation of the transfusion treatment should be a priority in order to rationalize the transfusion therapy. At each transfusion, pre and post transfusion Hb should be recorded, the weight and hematocrit of the blood transfused should be monitored. Serum ferritin, liver function tests, growth monitoring, cardiac and endocrinal evaluation should be done at regular intervals. A chart as shown in Fig. 1 should be maintained for each child. Important transfusion indices should be calculated yearly. The most useful indicators of appropriate management are: (i) Annual mean Hb level: Average of the mean pre and mean post transfusion Hb. (ii) Annual pure red cell consumption (ml/kg/year) Total wt (g) of blood given X Mean hematocrit (%) = _________________________________________ Patient's body weight (in mid-year) X 1.08* (*represents density of pure red cells)
Fig.1. Paitent Record Annual pure red cell consumption should not exceed 180 ml or a maximum of 200 ml/kg/yr. An increased value indicates development of hypersplenism or red cell antibodies. B. Iron Chelation Iron overload occurs from two sources namely transfused blood and enhanced gastro-intestinal tract iron absorption. Cumulative iron stores are also related to number of transfusions. Each unit of packed red cells provides 200-250 mg of iron and by 10 years of age about 20-30 g iron gets deposited in various parts of the body. Iron overload leads to liver fibrosis, cardiomyopathy and dysfunction of endo- crine organs. Without iron chelation, a well- transfused thalassemia patient dies between the age group of 10-25 years, ususally secondary to cardiac failure. There are various means by which iron overload can be estimated: (a) Serum ferritin estimation is the easiest and most widely used method of evaluating iron overload. Mean serum ferritin levels directly correlate with the cardiac status of the patient. Six monthly estimation of serum ferritin is recommended for appropriate monitoring of iron stores(4). However it is now being recognized that reliance on this test alone may lead to errors in management; changes in body iron account for little more than half the variation in serum ferritin concentrations(10); (b) Hepatic iron content can be assessed from biopsied liver tissue. The measurement of hepatic iron store, whose concentrations have been shown to correlate highly with total body iron stores, provide the most quantitative, specific, and sensitive method of evaluating iron burden in thalassemic patients(11). Determinations of hepatic iron concentrations from biopsied liver tissue obtained with ultrasonographic guidance is safe and permits rational adjustments in iron chelating therapy(12). Being an invasive proce-dure this is not routinely done; (c) Superconductive Quantum Interference Device (SQUID) biosusceptometry is another reliable noninvasive method of monitoring iron stores(13). However, this facility is not easily available; (d) Magnetic resonance imaging (MRI) can also be used to evaluate iron overload though the results are not very accurate(14). Out of a variety of iron chelating agents only Inj. desferrioxamine and an oral iron chelator (deferiprone) have been shown to be clinically effective with acceptable toxicity. Desferrioxamine Desferrioxamine (DFO), in use for the last 40 years, increases iron excretion both in urine and stool. Chelation treatment, which maintains ferritin <2500 mcg/l and hepatic iron concentration <268 mmol/g of dry weight liver, has been shown to enhance survival rates. Children with serum ferritin <2500 mcg/l have cardiac disease free survival of 91% after 15 years compared to 20% in those with higher serum ferritin values (6,7,15). One gram of desferrioxamine binds with 85 mg of iron. A daily excretion of more than 30-40 mg of iron can be achieved provided the drug is given 5 days a week. The optimal age at which chelation should be started is uncertain. While hepatic fibrosis sets in within two years of starting transfusion therapy, metaphyseal dysplasia has been reported before the age of three years. To be most effective, chelation therapy should be initiated only after iron accumulation is established, which is usually within 18 months of starting regular transfusions(16). By this time child would have received about 20-30 transfusions. This is usually associated with ferritin levels in the range of 800-1000 mcg/l. The daily dose of desferrioxamine is 40-60 mg/kg given subcutaneously over 8-10 hours. Vitamin C in a dose of 100 to 200 mg given during infusion helps in increasing iron excretion(17) and achieves negative iron balance relatively early. The infusion is usually given at home with a portable battery operated pump at night for 5-7 days per week. However, infusion pumps are costly and unaffordable by many patients in developing countries. A recent study evaluated the effectiveness of twice daily subcutaneous injections in place of prolonged infusion(18). Though this approach might be useful for developing countries further validation is necessary. Continuous intravenous infusions using surgical implants (portacath) is indicated for patients who are heavily iron loaded with adverse effects, for example, cardiac problems. These implants can also be used for regular transfusions thus avoiding repeated venepunctures. In general, the goal is to keep the serum ferritin level below 1000 mcg/ l. Levels above 7000 mcg/l interfere with growth and prolonged survival. Side effects of des-ferrioxime are mostly local irritation at injection sites and febrile reactions, which respond well to antihistaminics and antipyretics. The most feared side effect is infection with Yersinia enterocolitica and severe mucormycosis. Uncommon long-term toxicities include oto-toxicity and ocular toxicity. These patients should be regularly monitored for retinal changes, cataract and hearing problems. Oral Iron Chelators Regular subcutaneous desferrioxamine therapy is very costly and being cumbersome is available to less than 10% patients worldwide and less than 3% patients in India(19). Thus there is definite need for an effective oral iron chelator. Over last 30 years, hundreds of iron chelators have been tested in vitro or in animals. Out of these, only deferiprone was found to be reasonably effective to justify its licensing for general use in few countries. India is the first country, which has started licensing deferiprone for use (Kelfer-Cipla). Deferiprone is rapidly absorbed when ingested orally and when given in two or three doses daily, it causes iron excretion comparable to that caused by an equivalent daily dose of desferrioxamine over 8-10 hours. Effectivity of deferiprone over long term has also been shown in recent trials. A dose of 75 mg/kg/day divided into three subdoses, each given one hour before food is usually satisfactory. Serious side effects include agranulocytosis (1.8%) and arthropathy (20%) which necessitate discontinuation of the therapy. Gastrointestinal intolerance, zinc deficiency and fluctuations of liver functions are other side effects, which are reversible and transient in nature(20-22). Patients taking deferiprone should be monitored by blood counts 3-4 weekly and the drug should be discontinued if counts fall or severe joint pains and swelling occur with no relief to NSAIDs. However, data from two different centers showed that during long-term therapy in approximately 40% of patients, body iron burden stabilizes at or increases to concentrations associated with increased risk of cardiac disease, hepatic fibrosis and early death suggesting that long term deferiprone may not provide adequate control of body iron in a substantial number of patients(23). Research in Iron Chelation A combination of deferiprone and des-ferrioxamine has proved additive with a shift to urinary iron excretion. A depot formulation of desferrioxamine as a decane sulphonate salt suspended in Migliol 812 has been shown to have plasma kinetics 3-4 times longer than DFO in phase 1 trials. The duration of action is 3 to 6.5 days. Thus, this drug has the prospect of being used as subcutaneous injection once every 2-3 days. Another drug, in which DFO is linked to a hydroxy-ether starch polymer, HES-DFO has a half life 10-30 times longer than that of DFO, but the drug has disadvantages of instability and allergic reactions. Among oral chelators, a novel tridentate compound (ICL 670 A) has been shown to have highly selective and highly effective iron chelation. Another oral chelator pyridoxal isonicotinoyl hydrazone (PIH) has been shown to have high iron chelation efficacy and is relatively less toxic and more economical than deferiprone in animal studies(24). These experimental drugs require long term studies in humans. Splenectomy Splenectomy is usually not needed if regular transfusion therapy is followed. If the child already has a big spleen, his transfusion requirement increases to more than 1.5 times of the normal or more than 200 ml packed red cells or over 400 ml of whole blood per kg per year, splenectomy is indicated(4). Other indications are development of leukopenia, thrombo- cytopenia related to hypersplenism or massive splenomegaly causing discomfort. After splenectomy there may be transitory or persis-tent thrombocytosis. As a rule this carries no risk to the patient, possibly because it is simulta-neously balanced by reduction in platelet aggregation. However, aspirin 50 mg/day may be recommended for patients whose platelet count exceeds 800,000/cu mm. All patients should be vaccinated against Pneumococcus, Haemophilus influenzae b and Meningococcus before splenectomy is done. Chemoprophylaxis in form of oral penicillin V or intramuscular benzathine penicillin should be given for at least 2 years after splenectomy. However, it is desirable that penicillin pro-phylaxis should continue life-long. Parents should be educated to be aware of rapid onset of serious infections in such patients(25). Bone Disease in Beta Thalassemia Bone disease is an increasingly recognized cause of serious morbidity in thalassemic patients(26). Often it is detected late and efforts to prevent it and detect it early will reduce morbidity substantially. Patients commonly present with bone deformities, scoliosis, chronic bone pain, osteoporosis, fractures, growth failure, or nerve compression. Failure to achieve a peak bone mass, normally during late adolescence, and subsequent excessive bone resorption are important factors contributing to low bone mass(27). Osteopenia correlates strongly with gonadal failure and delayed puberty(28). Nutritional deficiencies, endocrine failure (hypothyroidism, hypoparathyroidism, diabetes, hypogonadism), desferrioxamine toxicity, persistent bone-marrow expansion, iron induced bone injury and inadequate exercise are the main contributing factors(29-31). Genetic factors also have an important influence on bone mass; Spl polymorphism in the COLIAI gene, which encode bone collagen and which has a strong association with low bone density, is prevalent among beta thalassemic patients (27,32). Prevention and treatment of early loss of bone mineral density are the best therapeutic options for controlling osteoporosis. Good nutrition with adequate vitamins and trace elements, along with calcium and vitamin D supplementation, can increase bone density and prevent bone loss. In adolescents, adequate calcium intake during skeletal development can increase the reserves for future bone resorption. Particular attention needs to be given to treatment of gonadal dysfunction(26,27). Hormone replacement therapy is beneficial for preventing bone loss and fractures though the risk involved in the treatment needs to be taken into consideration. For accurate assessement of blood requirement, hemoglobin concentration and reticulocyte count may not be very sensitive. Diagnostic tools such as serum concentration of transferrin receptors and erythropoietin can better define erythroid activity and transfusion requirement and minimize excessive marrow hyperplasia. Both over-chelation and under-chelation can adversely affect bone density and hence accurate assessment of body iron burden by measurement of hepatic iron status is important. Early diagnosis and treatment of glucose intolerance for prevention of loss of bone mass has recently been highlighted(33). Diets and Vitamins No strict regulations regarding diet can be recommended. However, food with rich iron content e.g., meat, liver, kidney, green leafy vegetables and jaggery, should be avoided. Food and water storage in iron utensils should be discouraged and prescriptions of iron containing medications must be avoided. Diet should include food high in phosphorous or phytates e.g., cereals, bread, milk, moong dal, soya beans, roasted peas, etc. to inhibit iron absorption, Similarly, strong tea having tannins may be taken alongwith or within an hour after meals to reduce iron absorption(34,35). Vitamin C facilitates iron chelation with DFO and should be supplemented in patients receiving DFO (5 mg/kg/d maximum of 200 mg/d). However in unchelated patients a low Vitamin C status is beneficial. Therefore citrus fruits, guava, amla, etc. which are rich in Vitamin C should be avoided. Food with high Vitamin C content should preferably be taken after cooking to reduce Vitamin C content(17,36). Folic acid (5 mg per week) should be given to patients receiving no or irregular transfusions. This is because of relative folate deficiency due to increased folate consumption. However, patients receiving regular blood transfusions ordinarily do not require folic acid unless actual deficiency state exists. C. Bone Marrow Transplantation Bone marrow transplantation (BMT) is at present the only cure for thalassemia major and is an accepted therapeutic alternative to lifelong regimen of blood transfusion and chelation. In BMT, the patients' bone marrow is first destroyed by drugs in a process called `conditioning'. Marrow is then harvested from a histocompatible donor and infused intravenously into the patient. The stem cells from the donor find their way into the marrow cavity and start growing there. As these stem cells have come from a normal person the red cells that are produced will also be normal. Since 1982, when first marrow transplant for thalassemia major was performed in 1981 at Seattle, USA(37), more than 1000 patients have been transplanted, the largest experience being at Pesaro, Italy(38,39). The cure rate of BMT is about 70%. In India, at present BMT for thalassemia is being done only at Vellore and the results are comparable with western centers (40). For BMT, patients are now-a-days categorized into three prognostically useful classes with respect to three risk factors, namely, poor quality of chelation, presence of hepato-megaly and the presence of portal fibrosis(41). Class I patient has no risk factor, Class II has one or two and Class III has all. In countries, where it is available, marrow transplantation should be considered for all patients with a suitable donor who falls into Class I or II. However, since the patients in Classes I and II already have a good prognosis with modern conventional management, the patients should be explained the risks and benefits of BMT versus conventional management. The results of marrow transplantation are improving steadily, with major progress in the management of transplant related complications. This is because of the use of cyclosporine, effective treatment for cytomegalovirus infection, better aseptic techniques and evolution of systemic antibiotic therapy. At the moment a patient in Class I has only a 5% probability of mortality(42). The best results in BMT can only be obtained with a matched sibling donor. The probability of finding an HLA identical sibling is 30%. The chance of finding an unrelated HLA identical donor is extremely rare. However, use of unrelated donor marrow registries has made the procedure somewhat less difficult. An Asian Indian Donor Marrow Registry has recently been established at AIIMS, New Delhi(43). Peripheral Blood Stem Cell Transplantation In this technique, stem cells are collected from peripheral blood of the donor by stimulating the release of stem cells from marrow to blood by use of certain drugs and growth factors(44). The advantages are easier processing, less expensive, faster marrow recovery and lower risk of graft versus host disease (GVHD), rejections and infections. However, there is always a concern for the adverse effects of cytokines and growth factors, which need to be administered to the healthy donor(45). Cord Blood Stem Cell Transplantation Cord blood contains hematopoietic stem cells that can be used for transplantation. Attempts to capitalize this source have been fruitful, as evidenced by the high success rate. Advantages are easy availability, less stringent requirement for HLA matching and lesser incidence of GVHD((46,47). However, most of these transplants have been carried in patients of leukemia and data regarding its utility in thalassemia is scarce. In utero Transplantation of Thalassemia This is based on the logic that any disease that can be prenatally diagnosed and is treated by BMT after birth could be treated by in utero transplantation. As in early fetal life new sites for hematopoiesis are constantly forming and are being occupied by migrating hematopoietic stem cell (HSC), engraftment of donor HSC is also possible on a competitive basis. Immuno-logical tolerance is another major advantage at this stage. Even with a low level of engraftment it is possible to clinically ameliorate the disease considerably. Experience in treating hemo-globinopathies with in utero transplantation is at present extremely limited(48). D. Gene Therapy Since, thalassemias are characterized by defective synthesis of globin subunits caused by mutations affecting gene regulation or expression, gene therapy remains the ultimate treatment for providing a lifelong cure. In this mode of therapy, patient's bone marrow is harvested and beta globin gene is incorporated into stem cell and reinfused in the body system. The critical factor in gene therapy is an appropriate level of gene expression. Substantial progress has been made in recent years to improve the gene expression by using retroviruses as vectors(49,50). These viruses have ability to multiply and encode foreign nucleic acid and contain mechanism for chromosomal integration. Non viral vectors like bacterial artificial chromosome, yeast artificial chromosome, and human artificial chromosome are exciting prospects for the future(51-53). It is difficult to foresee the time when an efficient gene therapy will be available in reducing the burden of both the disease and its current treatment! E. Stimulation of Fetal Hemoglobin Synthesis Increased gamma globin chain synthesis will reduce the imbalance of alpha chains and hemolysis. Several drugs like hydroxyurea, butyrates, 5-azacytidine, cytosine arabinoside, vinblastine, and busulphan have been shown to increase Hb F synthesis. Therapy with hydroxy-urea and butyric acid compounds seems to be promising as it neutralizes the noxious excess of alpha chains and allows a better survival of the erythroid precursors in the marrow and of the red cells in the peripheral blood. Hydroxy-urea has been used in daily dose of 10-20 mg/kg varying from 4-30 weeks. The drug is well tolerated and its main toxicity, i.e., leukopenia and thrombocytopenia is fully reversible(54-58). However, other studies, have reported only small increases in fetal and total hemoglobin concentrations during the administration of these compounds(59-60). Heme arginate, a novel stable form of hemin has shown to increase Hb levels in few thalassemic patients(61). Recombinant erythropoietin increases recruitment of progenitor cells, some of which produce more gamma globin chains. However, it has been mainly tried in thalassemia intermedia cases(62,63). Despite the increase in the design and implementation of therapies aimed at the augmentation of fetal hemoglobin synthesis in beta thalassemia, their use in thalassemia major is still in its infancy. It is likely that combination therapies may prove useful in the augmentation of fetal hemoglobin sufficiently enough to decrease transfusion requirements. Studies to evaluate the effective-ness of combination therapies in patients with thalassemia are continuing. Thalassemia Intermedia The term thalassemia intermedia applies to persons with a clinical thalassemia syndrome, who remain well without transfusion (at least early in life). Differentiation from thalassemia major has already been alluded to. Patients with thalassemia intermedia may need occasional blood transfusion because the hemoglobin can drop temporarily, sometimes below 7g/dl, especially in relation to infection. Hyper-splenism can lead to a persisting fall in hemoglobin level mimicking thalassemia major. In such case, the appropriate management is splenectomy, rather than starting on mainte-nance transfusion. Patients who can lead a normal life and maintain hemoglobin of 8 g/dl should not be started on regular transfusions. Persistent clinical problems such as pathological fractures, growth retardation, masses of ectopic marrow or cardiac failure are absolute indicators for regular transfusions. Once a decision is taken to start maintenance transfusion, the scheme should be same as that for thalassemia major. Pregnant women with thalassemia intermedia should be transfused throughout pregnancy. Even nontransfusion dependent thalassemic patients develop iron overload as a result of increased gastrointestinal iron absorption and occasional transfusions. Iron rich foods should be avoided and a cup of tea with meals may be advised. Principles of chelation therapy and splenectomy are the same as in the case of thalassemia major. Non transfusion dependent thalassemic should be given folic acid 4 mg/week orally due to excessive requirements because of continuing hemolysis. Carrier screening and prenatal diagnosis of the beta thalassemias is the most effective approach to reduce the incidence of the disease. This has already been discussed in the preceding issue of the journal(64). Key Messages
References 1. Weatherall DJ, Clegg JB. Thalassemia-a global public health problem. Nat Med 1996; 2: 847-849. 2. Olivieri NF. The B-Thalassemias. N Engl J Med 1999; 341: 99-109. 3. Marwah RK, Lal A. Present status of hemoglobinopathies in India. Indian Pediatr 1994; 31: 267-271. 4. Management Protocol for Treatment of Thalassemia Patients. Cyprus, Thalassemia International Federation, 1997. 5. Cao A, Galanello R, Rosatelli MC, Argiolu F, Virgilils SD. Clinical experience of management of thalassemia: the Sardinian experience. Semin Hematol 1996; 33: 66-75. 6. Olivieri NF, Nathan DG, Macmillan JH, Wayne AS, Liu PP, McGee A, et al. Survival in medically treated patients with homozygous beta thalassemia. N Engl J Med 1994; 331: 574-578. 7. Olivieri NF, Brittenham GM. Iron chelating therapy and treatment of thalassemia. Blood 1997; 89: 739-761. 8. Kumar RM, Riak DE, Khurana A. Beta thalassemia major and successful pregnancy. J Reprod Med 1997; 42: 294-298. 9. Sirchia G, Wenz B, Rebulla P. Removal of white cells from red cells by transfusion through a new filter. Transfusion 1990; 30: 30-33. 10. Brittenham GM, Cohen AR, McLaren CE, Martin MB, Griffith PM, Nienhuis AW et al. Hepatic iron stores and plasma ferritin con-centration in patients with sickle cell anemia and thalassemia major. Am J Hematol 1993; 42: 81-85. 11. Angelucci E, Giardini C, Brittenham GM Lucarelli G. Hepatic iron concentrations and body iron stores determined by quantitative phlebotomy in patients cured of thalassemia major by bone marrow transplantation. Blood 1997; 90: (Suppl 1): 265 a. abstract. 12. Olivieri NF, Brittenham GM. Iron chelating therapy and the treatment of thalassemia. Blood 1997; 89: 739-761 [Erratum, Blood 1997; 89: 2621]. 13. Brittenham GM, Farrel DE, Harris JW. Magnetic susceptibility measurements of human iron stores. N Engl J Med 1982; 307: 1671-1675. 14. Mazza P, Gida R, De Moxo S, Bonetti MS, Amerri B, Magi C. Iron overload in thalassemia: Comparative analysis of magnetic resonance imaging, serum ferritin and iron content of the liver. Hematologica 1995; 80: 398-404. 15. Brittenham GM, Griffith PM, Nienhaus AW, Mclaren CE, Tucker EE, Alen CJ, et al. Efficacy of desferrioxamine in preventing complications of iron overload in patients with thalassemia major. N Engl J Med 1994; 331: 567-573. 16. Lucarelli G, Giardini C, Baronciani D. Bone marrow transplantation in thalassemia. Semin Hematol 1995; 32: 297-303. 17. Sharma BK, Choudhury P, Dubey AP. Desferrioxamine: It's use in iron chelation in thalassemia. Indian Pediatr 1990; 27: 314-319. 18. Borgna PC, Cohen A. Evaluation of a new method of administration of the iron chelating agent desferrioxamine. J Pediatr 1997; 130: 86-88. 19. Aggarwal MB. Living with Thalassemia. Bombay, Bhalani Book Depot, 1986. 20. Kontoghiorges GJ, Aldouri MP, Hoffbrand AV, Barr J, Wonke B, Kourouclaris T, et al. Effective chelation of iron in thalassemia with the oral chelator 1,2-dimethyl-3-hydroxypyrid-4-one. BMJ 1987; 295: 1509-1512. 21. Agarwal MB, Gupte SS, Vishwanathan C, Vasandani D, Ramanathan J, Desai N, et al. Long term assessment of efficacy and safety of L1, an oral iron chelator in transfusion dependent thalassemia: Indian trial. Br J Hematol 1992; 82: 460-466. 22. Al-Refaie FN, Hershko C, Hoffbrand AV, Kosaryan, Olivieri, NF, Tondury P, et al. Results of long term deferiprone (L1) therapy: A report by the International Study Group on oral iron chelators. Br J Hematol 1995: 91: 224-229. 23. Olivieri NF. Thalassemia today. Acta Hematologica 1998; 100 (Suppl 1): 9. 24. Piga A, Longo I, Voi V, Facello S, Tartaglia N. Advances in iron chelating therapy. Acta Hematologica 1998; 100 (Suppl 1): 270. 25. Williams DN, Kaur B. Postsplenectomy care: Strategies to decrease the risk of infection. Postgrad Med J 1996; 100: 195-205. 26. Jensen CE, Tuck SM, Agnew JE, Koneru S, Morris RW, Yardumian A, et al. High prevalence of low bone mass in thalassemia major. Br J Hematol 1998; 103: 911-915. 27. Filosa A, Di Maio S, Vocca S, Saviano A, Esopotito G, Pagono L. Longitudinal monitoring of bone mineral density in thalassemia patients: Genetic structure and osteoporosis. Acata Pediatr 1997; 86: 342-346. 28. Roth C, Pekrun A, Bartz M, Jarry H, Eber S, Lakomek M, et al. Short stature and failure of pubertal development in thalassemia major: Evidence hypothalamic neurosecretory dysfunction of growth hormone secretion and defective pituitary gonadotrophin secretion. Eur J Pediatr 1997; 156: 777-783. 29. Filosa A, Di Maio S, Saviano A, Vocca S, Esposito G. Can adrenarche influence the degree of osteopenia in thalassemic children? J Pediatr Endocrinol Metab 1996; 9: 401-406. 30. De Sanctis V, Pinamonti A, Di Palma A, Sprocati M, Ahi G, Gamberini MR, et al. Growth and development in thalassemia major patients with severe bone lesions due to desferrioxamine. Eur J Pediatr 1996; 155: 368-372. 31. Pafuni C, Roccasalva L, Pernicone G, Spano G, Palumbo MA, Gregorio FD, et al. Osteopenia in female beta-thalassemic patients. J Pediatr Endocrinol metab 1998; 11: 989-991. 32. Wonke B, Jensen C, Hanslip JJ, Prescott E, Lalloz M, Layton M, et al. Genetic and acquired predisposing factors and treatment of osteoporosis in thalassemia major. J Pediatr Endocrinol Metab 1998; 11: 795-801. 33. Singer ST, Vichinsky EP. Bone disease in beta thalassemia (Commentary). Lancet 1999; 354: 881-882. 34. DeAlarcan PA, Donovan ME, Foebes GB, Landau SA, Stockam JA. Iron absorption in the thalassemia syndromes and its inhibition by tea. N Engl J Med 1979; 300: 5-8. 35. Disler PB, Lynch SR, Charton RW, Torrance JD, Bothwell TH, Walker RB, et al. The effect of tea on iron absorption. Gut 1975; 16: 193-200. 36. Singh J, Mangal NK, Khinchi YR. Diet in regularly transfused thalassemics. Indian Pediatr 1994; 30: 1453-1456. 37. Thomas ED, Buckner CD, Sanders JE. Marrow transplantation for thalassemia. Lancet 1982; 2: 227-229. 38. Lucarelli G, Clift RA, Galinberti M, Polchi P, Angelucci E, Baronciani D, et al. Marrow transplantation for patients with thalassemia: Results in class 3 patients. Blood 1996; 87: 2062-2088. 39. Piomelli S. Cooley's anemia management: 25 years of progress. In: Advances and Controversies in Thalassemia Therapy: Bone Marrow Transplantation and Other Approaches. Eds. Buener CD, Gale RP. Lucarelli G. New York, Alan R Liss, 1989; pp 23-26. 40. Chandy M. Bone marrow transplantation for thalassemia. In: Proceedings of 2nd National Thalassemia Conference, New Delhi, 1997; pp 61-66. 41. Lucarelli G, Galimberti M, Polchi P, Angelucci E, Baronciani D, Giardini C, et al. Bone marrow transplantation in patients with thalassemia. N Engl J Med 1990; 322: 417-421. 42. Giardnini C, Lucarelli G, Galinberti M, Baronciani D, Angelico E, Polchi P, et al. Bone marrow transplantation in thalassemia. Acta Hematologica 1998; 100 (Suppl 1): 284. 43. Mehra NK. Asian Indian Donor Marrow Registry. In: Proceedings of 2nd National thalassemia Conference 1997, New Delhi, 1997; 58-60. 44. Ossenkoppele GJ, Jonkoff AR, Huihgens PC, Nauta JJP, Vander HKG, Drager AM. Peripheral blood progenitor cells mobilized by G-CSF (Filgrastim) and reinfused as unprocessed autologous whole blood shorten the pancytopenic period following high dose melphalan in multiple myeloma. Bone marrow Transplant 1994; 13: 37-41. 45. Choudhry VP. Hematopoietic Stem cell transplantation. Indian Pediatr 1997; 34: 505-517. 46. Silberstein LE, Jefferies LC. Placental blood banking. A new frontier in transfusion medicine. N Engl J Med 1996; 335: 199-201. 47. Kurteber J, Laughlin M, Graham ML, Smith C, Olsan JF, Halperin EC, et al. Placental blood as a source of hematopoietic stem cell for transplantation into unrelated recipients. N Engl J Med 1996; 335: 157-166. 48. Westgren M, Ringden O, Eik-Nes S, Ek S, Anvret M, Brubakk AM, et al. Lack of evidence of permanent engraftment after in utero fetal stem cell transplantation in congenital hemoglobinopathies. Transplantation 1996; 61: 1176-1179. 49. Leboutch P, Huang GS, Humphires RK. Mutagenesis of retroviral vectors transducing beta globin gene and beta globin locus control region derivates results in stable transmission of an active transcriptional structures. EMBO J 1994; 13: 3065-3076. 50. Beuzard Y. Towards gene therapy of hemoglobinopathies. Semin Hematol 1996; 33: 43-52. 51. Harrington SJ, Van Bokklen G, Mays RW. Formation of de novo centromeres and construction of first generation human artificial microsomes. Nature Genetics 1997; 4: 345-355. 52. Loqnnou PD, Amemiya CT, Garnes J, Kroisel PM, Shizuya H, Chen C, et al. A new bacteriophage P1 desired vector for the propagation of large human DNA fragments. Nature Genetics 1994; 6: 84-89. 53. Rivella S, Sadelain M. Genetic treatment of severe hemoglobinopathies: The combat against transgene variegation and transgenic silencing. Semin Hematol 1998; 35: 112-125. 54. Perrine SP, Ginder GD, Faller DV, Dover GH, Ikuta J, Witkowska HE, et al. A short term trial of butyrate to stimulate fetal globin gene expression in the beta-globin disorders. N Engl J Med 1993; 328: 129-131. 55. Faller DV, Perrie SP. Butyrates in the treatment of sickle cell disease and beta thalassemia, Curr Opin Hematol 1995; 2: 109-117. 56. Choudhry VP, Lal A, Pati HP, Arya LS. Hematological responses to hydroxyurea therapy in multi transfused thalassemic children. Indian J Pediatr 1997; 64: 395-398. 57. Arruda VR, Lima CSP, Saad STO, Costa FF. Successful use of hydroxyurea in B-thalassemia major. New Engl J Med 1997; 336: 964. 58. Olivieri NF, Rees DC, Ginder GD, Thein, Brittenham GM, Waye JS, et al. Treatment of thalassemia major with phenylbutyrate and hydroxyurea. Lancet 1997; 350: 491-492. 59. Rodgers GP, Rachmilewitz EA. Novel treatment options in the severe B-globin disorders. Brit J Hematol 1995; 91: 263-268. 60. Collins AF, Pearson HA, Giardina P, McDonagh KT, Brusilow SW, Dover GJ. Oral sodium phe-nylbutyrate therapy in homozygous beta thala-ssemia: A clinical trial. Blood 1995; 85: 43-49. 61. Rind D, Fibach E, Goldfar BA, Friedbarg A, Rachmilewitz EA. Heme arginate therapy for beta thalassemia: in vitro versus in vivo effects. Acta Hematol 1998; 100: 82-84. 62. Rachmilewitz EA, Goldfarls A, Dover G, Administration of erythropoietin to patients with beta thalassemia intermedia: A preliminary trial. Blood 1991; 78: 1145-1147. 63. Olivieri NF, Freedman M, Perrine S, Dover GJ, Sheridan B, Essentine DL, et al. Trial of recombinant human erythropoietin in thalassemia intermedia. Blood 1992; 80: 3258-3260. 64. Maheswari M, Arora S, Kabra M, Menon PSN. Carrier screening and prenatal diagnosis of b-thalassemia. Indian Pediatr 1999; 36: 1119-1125. |