|
Original Articles Indian Pediatrics 1999;36: 1211-1219 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Epidemiological characteristics of poliomyelitis in delhi, 1997 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Jagvir Singh,
Shashi Khare, Rajesh Bhatia, D.C. Jain and Jotna Sokhey From
the National Institute of Communicable Diseases, 22 Shamnath Marg, Delhi 110 054, India. Objective: To describe the epidemiological characteristics of poliomyelitis in Delhi in 1997 after four consecutive statewide immunization campaigns with oral polio vaccine (OPV). Methods: Stool samples were collected from 158 cases of acute flaccid paralysis (AFP) along with their age, sex, residential address, immunization history and dates of onset of paralysis, reporting and investigation. The samples were processed for isolation of polioviruses. In addition, historical data on vaccination coverage surveys and OPV testing were reviewed. These data were analyzed to understand the epidemiological patterns of poliomyelitis in Delhi. Results: Of 158 cases of AFP, about 23% were investigated within 2 days of onset of paralysis. Two samples each were collected from 97 (61%) cases, and one each from the remaining cases. Detection of 158 cases of AFP gave an incidence of 1.34 per 100,000 population. About 36% (57/158) of AFP cases excreted poliovirus, mostly (53/158) wild poliovirus. Of the wild poliovirus isolates, 72% (38/53) and 25% (13/53) were serotypes P1 and P3 respectively; 2 isolates were P2. Almost 95% (146/154) of AFP cases and all the laboratory confirmed cases (excreting wild poliovirus) occurred in children below 5 years of age. Only one-third of AFP (55/158) or laboratory confirmed cases (18/53) had received 3 or more doses of OPV before onset of paralysis. About one-fourth of cases in both the categories were totally unvaccinated. AFP cases occurred round the year but peaked in November-December. Peaks were always observed during July-August in the past. The cases were widely scattered without any obvious clustering in any locality. Conclusions: Poliomyelitis has declined substantially in Delhi. The study underscores the need for further efforts to improve vaccine coverage levels, AFP surveillance, and cold chain maintenance to achieve the complete interruption of transmission. Key words: Acute flaccid paralysis, Cold chain, Oral polio vaccine, Poliomyelitis. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
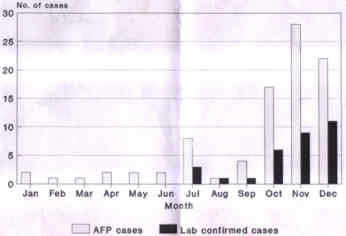
Oral polio vaccine (OPV) was introduced in the Expanded Programme on Immunization (EPI) in India in 1979. Reported coverage with 3 doses of OPV increased from about 30% in 1985-86 to about 90% in 1990s(1). Commensurate with the increase in OPV coverage levels, the estimated incidence of polio declined from about 25 per 100,000 population in the pre-immunization era to about 16 per 100,000 population in 1989 and to about 6 per 100,000 population in 1992(2-4). While high routine immunization coverage levels can reduce the incidence of polio significantly, experience in many countries has shown that the addition of National Immunization Days (NIDs) and surveillance of acute flaccid paralysis (AFP) is necessary to interrupt wild virus transmission and to achieve eradication of poliomyelitis(5). Delhi was the first state in India to adopt this strategy(6). All the children below 3 years of age were offered OPV on 2 October and 4 December 1994 irrespective of previous history of immunization. It was called Pulse Polio Immunization (PPI). The age limit remained the same in the next campaign(7), but was increased to 5 years in the two subsequent campaigns. This paper reviews the polio situation in Delhi in 1997, after four consecutive PPI campaigns have been conducted. Subjects and Methods Background of poliomyelitis in Delhi Delhi, the capital of India, has a population of more than 9 million (1991 census) with an average population density of around 6350 per sq km. For more than 4 decades, the population has been growing rapidly, at a constant rate of about 50% per decade. More than 25% of the population live in slums that do not have access to sewerage and use water from shallow tube wells for drinking, cooking and other domestic purposes. Poliomyelitis has been a major public health problem in Delhi. Cases occur throughout the year with peaks during July and August, which are summer and monsoon months in Delhi(8,9). About 85% of the cases occur in children below 3 years of age(10). More than 80% of cases reported in Delhi are seen at the Kalawati Saran Children Hospital (KSCH) which is known for its expertise in the management of poliomyelitis and therefore, acts as sentinel centre for poliomyelitis in Delhi(9). Cases from this hospital and other health agencies are reported to and investigated by the Directorate of Family Welfare and Municipal Corporation of Delhi. Methods In 1997, stool samples were collected from 158 cases and transported in the reverse cold chain along with patient name, age, sex, residential address, immunization history and dates of onset of paralysis, reporting and investigation of cases and collection of stool samples_to the Laboratories of National Institute of Communicable Diseases (NICD), Delhi, which act as WHO Regional Poliovirus Reference Laboratory. Unfortunately, the vital dates were not mentioned in many forms. Each sample after pre-treatment was subjected to virus isolation on RD and Hep2 cell lines as per WHO guidelines(11). The isolates were typed as poliovirus type 1, 2, 3, or mixture using standard techniques and antisera procured from RIVM, Netherlands. All the poliovirus isolates were subjected to intratypic differ-entiation by ELISA technique using cross-absorbed rabbit antisera and RNA probe hybridization technique. Reagents for ELISA were procured from RIVM, Netherlands, and for RNA probe hybridization from Molecular Virology Laboratory, CDC, Atlanta, USA. For hybridization procedure, 2 types of probes, i.e., group probe and poliovirus genotype specific Sabin probe, were used. In this technique, Sabin related strains were directly identified using Sabin strain specific probe. Wild polioviruses were recognized by the inability of their genomes to form stable hybrid with the Sabin strain specific probes. As per WHO criteria, the isolates were interpreted as Sabin or wild after testing by ELISA and RNA probe techniques. A person was considered positive for wild poliovirus if wild poliovirus was isolated from either or both the stool samples and on any of the cell lines used. All the routine or PPI doses of OPV received one month before onset of paralysis were considered to classify a case as partially (1 or 2 doses) or fully (3 or more doses) vaccinated. Using the standard WHO 30-cluster sampling technique many vaccine coverage surveys have been carried out in Delhi. Published as well as unpublished documents were screened to find out OPV coverage levels from 1988 through 1996(3,12,13). Data on OPV potency testing from Delhi were collected from the laboratories of NICD. Data on population required to calculate the incidence of AFP were based on estimates by the Registrar General of India after making adjustment for population changes during 1991-97. Epi Info software version 6.02 was used for analysis of data. Results Overall stool samples of 158 cases of AFP were received in NICD in 1997. This gave an annual incidence of 1.34 per 100,000 population (or 11.2 per 100,000 under-five children). Most of the AFP cases occurred during the period from July to December. The peak was observed in November-December (Fig. 1). In contrast, peaks were always observed during July-August in the past. The cases were widely scattered without any obvious clustering in any locality.
Fig. 1 Seasonality of poliomyelitis in Delhi, 1997 About 36% (57/158) of AFP cases excreted poliovirus; one-third (53/158) excreted wild poliovirus, and 2% (3/158) excreted Sabin poliovirus. One poliovirus isolate could not be typed (Table I). About 72% (38/53) and 25% (13/53) of wild poliovirus isolates were serotypes P1 and P3 respectively. Two isolates each of wild and Sabin poliovirus were P2. Table I__ Isolation of Poliovirus in AFP Cases (n=158) in Delhi, 1997.
*P1=38, P2=2, P3=13., **P1=1, P2=2 The cases are described by age and immunization status in Table II and III. About 95% (146/154) of AFP cases and all the laboratory confirmed cases occurred in children below 5 years of age. The median age in the two groups was 18 and 12 months, respectively (Table II). Analysis of cases by immunization status revealed that only one-third of AFP (55/158) or laboratory confirmed cases (18/53) had received 3 or more doses of OPV before onset of paralysis. One-fourth of cases in both the categories had not received even a single dose of OPV (Table III). Table II__ AFP or Laboratory Confirmed Polio- myelitis Cases By Age.
Table III__ AFP or Poliomyelitis Cases by Immunization Status.
Table IV describes the indicators of AFP surveillance in Delhi in 1997. Appropriate data were not available for many cases. Only one-fourth (11/48) of cases were investigated by local health officials within 2 days of onset of paralysis. Two samples each were collected from 97 (61%) cases, the remaining 61 (39%) AFP cases provided one sample each. Overall 80% (91/114) of stool samples were collected within 2 weeks of onset of paralysis. Interval between two samples was 3 days or less in 88% (52/59) of cases. Table IV__Indicators of AFP Surveillance in Delhi, 1997.
Isolation rates of poliovirus in 97 cases from whom 2 stool samples each were collected are shown in Table V. About 37% (36/97) of these cases excreted poliovirus; 22 in both samples, 7 only in first samples, and 7 only in second samples. Table V__ Isolation of Poliovirus in First and Second Stool Samples in Delhi, 1997.
Positive = poliovirus isolated. ,Negative = poliovirus not isolated. Table VI__OPV Coverage Estimates in Surveys Conducted in Large Population Areas in Delhi.
Table VI shows OPV coverage levels (in the age group 12-23 months) estimated by coverage surveys carried out during 1988-96. Data on OPV potency testing from Delhi during 1989-97 are shown in Table VII. Table VII__ OPV Potency Testing in Delhi, 1989-97.
Discussion Based on the cases reported through routine surveillance system, it has been estimated that the incidence of poliomyelitis in Delhi declined from 15.7 per 100,000 population in 1975 to 5.9 per 100,000 population in 1992(14). In 1997, the annual incidence was 1.34 per 100,000 population, a reduction of more than 90% from the prevaccination era. Although the decline is impressive, what remains after four rounds of PPI campaigns is also substantial. This indicates use of a vaccine of sub-optimal efficacy and/or failure to achieve sufficiently high vaccine coverage levels in all the communities required to interrupt transmission of poliovirus. There was evidence to support both the possibilities. Vaccine coverage surveys carried out between 1988 and 1996 indicate that coverage levels with 3 doses of OPV were not uniformly high (Table VI). There were large areas with poor coverage levels. For example, coverage levels with 3 doses of OPV were only 53% in JJ colonies (slums constituting more than 1.2 million population) in 1990(13). In 1996, only 70% of infants in east Delhi (more than 2 million population) had received 3 doses of OPV. PPI campaigns also did not cover all areas or groups uniformly. A coverage evaluation survey undertaken in March 1996 revealed that 80% and 90% of the children received the first (December 1995) and second (January 1996) PPI dose, respectively. While overall 77% of the eligible children received both the doses, only 67% of the infants below 6 months of age received both the doses(7). These gaps in the vaccination coverage perhaps left many susceptible children who sustained transmission of poliovirus in the community. Although about 83% (2835/3428) Of OPV samples from Delhi were found to have satisfactory titre (106.15�0.5 TCID50 per 0.1 ml) from 1989 through 1997, only 76% (448/589) and 58% (264/454) of OPV samples were found to be potent in 1994 and 1996, respectively (Table VII). Obviously there are some problems in cold chain maintenance that need to be investigated and overcome by immediate corrective measures to achieve the goal of eradication of poliomyelitis. Even if the OPV vaccines are properly maintained in the cold chain, they do not prevent disease in all the recipients(15). Nearly one-third of AFP (55/158) or laboratory confirmed cases (18/53) had received 3 or more doses of OPV before the onset of paralysis (Table III). One would expect this proportion to increase as the coverage levels improve. In fact, proportion of cases found fully vaccinated increased from 2% (157/6503) in 1980-83 to 16% (798/5084) in 1988-91, and to 22% (739/3416) in 1992-94(8,9). These trends indicate improvement in the vaccine coverage over the years. A dramatic change in the seasonality of polio in 1997 may also be due to the effect of PPI campaigns, which were undertaken in December and January every year (Fig. 1). Nevertheless, occurrence of almost one-fourth of cases in totally unvaccinated children also indicates the need to improve the coverage levels further. As shown in Table II, poliomyelitis continued to affect mainly young children in Delhi. Almost 95% (146/154) of AFP cases and all the laboratory confirmed cases occurred in children below 5 years of age. The median age in two groups was 18 and 12 months, respectively. Thus, the age distribution of cases in 1997 did not differ from that observed in the prevaccination era in Delhi or other parts of country(10). The results confirmed our earlier suggestion that any major shift in age at onset of paralysis may not occur in India despite high coverage levels with OPV (unless there is concomitant improvement in sanitation and hygiene). The results also support that acute flaccid paralysis in children below 5 years of age provide a highly sensitive and specific case definition for acute poliomyelitis and that age limit of 5 years is appropriate for immunization campaigns in India. While immunization campaigns will reduce the incidence of poliomyelitis, a few foci of transmission will be maintained. The purpose of AFP surveillance_detection, reporting, investigation followed by outbreak response - is to identify and eliminate the remaining chains of transmission. Thus, AFP surveillance is the critical component of polio eradication strategy. We anlayzed the data to understand the present status of AFP surveillance in Delhi. Only one-fourth (11/48) of cases were investigated within 48 hours of onset of paralysis. To prevent the spread of infection in the community, it is essential that most of the cases are detected, reported and investigated within 48 hours of onset of paralysis. It is also envisaged that all cases should be investigated by collecting 2 stool samples (in reverse cold chain) at an interval of 24-48 hours within 14 days of onset of paralysis. Early collection of stool samples increases the possibility of poliovirus isolation. However, it was not done in more than 20% of the cases (Table IV). Two samples were collected from only 61% (97/158) of cases, and in only 66% (39/59) of such cases the interval between 2 samples was 24-48 hours. The fact that collection of 2 samples increases the possibility of isolation of poliovirus(16) was also evident from the data shown in Table V. Seven of 31 (23%) poliovirus isolates would have been missed in the absence of a second stool sample. Wild polioviruses were isolated from 34% (53/158) of AFP cases. It is difficult to say with certainty as to in how many cases poor specimen collection was responsible for failure to isolate poliovirus, or causes other than polio were responsible for AFP cases found negative for wild poliovirus. Nevertheless, it would not be proper to discard these AFP cases (who fail to excrete wild poliovirus) as non-polio. Opinion of an experienced physician who has examined the case at the onset of illness as well as the condition of child at 60 days follow-up should also be taken into account to classify a case of AFP as polio. If such data are not collected or available, all the cases of AFP should be considered and reported as polio. We do not have data on 60 days follow-up of these cases. However, the isolation of poliovirus from similar proportion (399/1221 = 33%) of clinically suspected cases of polio in Delhi or surrounding areas during 1992-94(17) and age distribution of AFP cases in 1997 (95% cases in under-five children) indicate that most, if not all, of the AFP cases in 1997 were perhaps due to poliomyelitis. Lastly, 3 AFP cases excreted only Sabin virus. At least 2 of them had received OPV vaccine between collection of stool samples and onset of paralysis. No information was available for the third case (10 months aged female) who provided only one sample. These patients were unlikely to have vaccine associated paralysis. In conclusion, polio has declined tremendously but continues to be a substantial problem in Delhi. Further efforts are necessary to improve vaccine coverage levels through routine services and PPI campaigns, and AFP surveillance to interrupt the transmission completely. Acknowledgements The authors are grateful to Mrs. Meena Datta of National Institute of Communicable Disease, Delhi for providing technical assistance for processing of stool samples. References 1. Ministry of Health and Family Welfare, Government of India. Annual Report 1996-97, pp 25-32. 2. Singh J, Foster SO. Sensitivity of poliomyelitis surveillance in India. Indian Pediatr 1998; 35: 311-315. 3. Gupta JP, Murali I. National Review of Immunization Programme in India. National Institute of Health and Family Welfare, New Mehrauli Road, New Delhi, 1989. 4. Ministry of Health and Family Welfare, Government of India. Review of the Universal Immunization Programme. Joint Report by the Government of India, WHO and UNICEF. Country Overview, September, 1992. 5. de Quadros CA, Andrus JK, Olive JM, de Macedo CG, Henderson DA. Polio eradication from the Western Hemisphere. Ann Rev Public Health 1992; 13: 239-252. 6. Bandyopadhyay S, Banerjee K, Datta KK, Atwood SJ, Langmire CM, Andrus JK. Evaluation of mass pulse immunization with oral polio vaccine in Delhi: Is pre-registration of children necessary? Indian J Pediatr 1996; 63: 133-137. 7. Singh B, Suresh K, Kumar S, Singh P. Pulse polio immunization in Delhi-1995-96: A survey. Indian J Pediatr 1997; 64: 57-64. 8. Sharma M, Sen S, Ahuja B, Dhamija K. Paralytic poliomyelitis 1976-1988: Report from a sentinel centre. Indian Pediatr 1990; 27: 143-150. 9. Ahuja B, Gupta VK, Tyagi A. Paralytic poliomyelitis (1989-1994): Report from a sentinel centre. Indian Pediatr 1996; 33: 739-745. 10. Singh J, Sharma RS, Verghese T. Epidemiological considerations on age distribution of paralytic poliomyelitis. J Trop Pediatr 1996; 42: 237-241. 11. Expanded Programme on Immunization. Manual for the Virological Investigation of Polio. WHO document WHO/EPI/GEN/97.01, 1997. 12. Varshney VP. Vaccination Coverage Evaluation Surveys, UT, Delhi, March 1988. Directorate of Health Services, Delhi Administration, New Delhi, 1988. 13. Chawla SC, Bachani D, Bansal RD. Vaccination Coverage of Infants and Mothers, Prevalence of Poliomyelitis and Incidence of Neonatal Tetanus in the Resettlement and J.J. Colonies of Delhi. Department of Preventive and Social Medicine, Lady Hardinge Medical College, New Delhi, 1990. 14. Bhattarcharjee J, Devadethan, Sharma RS. Acute paralytic poliomyelitis in Delhi (1975-1992). Indian J Pediatr 1994; 61: 167-172. 15. Patriarca PA, Wright PF, John TJ. Factors affecting the immuogenicity of oral poliovirus vaccine in developing countries: Review. Rev Inf Dis 1991; 13: 926-939. 16. Expanded Programme on Immunization. Maximizing poliovirus isolation rates. EPI Alert, July 1993, p 6. 17. Khare S, Bhatia R, Kumari S, Datta KK. Virologic surveillance of poliomyelitis in Delhi. Indian Pediatr 1996; 33: 746-750. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||