|
Case Reports Indian Pediatrics 1999;36:1259-1262 |
Mediastinal Yolk Sac Tumor_ A Rare Presentation |
Milind S. Tullu, Chandrahas T. Deshmukh, Pradeep Vaideeswar*, Burjor A. Bharucha, Priyanka K. Arora From the Departments of Pediatrics and Pathology*, Seth G.S.
Medical College and K.E.M. Hospital, Parel, Mumbai 400 012, Maharashtra, India. |
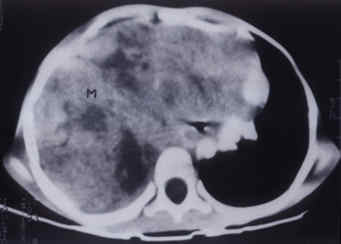
| Germ cell tumors are rare and occur with an incidence of approximately 2.7 per 106 person years(1). Yolk sac tumor (endodermal sinus tumor) is the most common malignant germ cell tumor found in the pediatric age group(2). These are generally seen in combination with other germ cell tumors and pure extragonadal yolk sac tumors are rare(2,3). Like other germ cell tumors, the commonest site for yolk sac tumors include the gonads(2,4). Other less common sites include the sacrococcygeal region, mediastinum, vagina, urinary bladder, liver, nasopharynx, posterior cranial fossa and face(2-10). We present a rare case of a mediastinal pure yolk sac tumor. Case Report A 3�-year-old-male child presented with moderate to high grade fever, non-productive cough and progressive breathlessness for the past two months. On general examination, the condition was unsatisfactory with tachycardia (heart rate - 126/min) and respiratory distress with intercostal retractions (respiratory rate - 60/min). There was no cyanosis or significant lymphadenopathy. On examination of the respiratory system, the trachea and the heart were shifted to the left side. The right hemithorax showed decreased movements, was stony dull on percussion and the air entry was markedly diminished. There was no hepato-splenomegaly or ascites. Chest radiograph revealed an opacity in the right hemithorax with sparing of the right costophrenic angle and the lateral view showed an anterior mediastinal mass. USG chest was suggestive of a hyperechoic mediastinal mass without calcifications. CT chest revealed a non-homogeneous enhancing anterior mediastinal mass extending into the right hemithorax and right lung (Fig. 1).
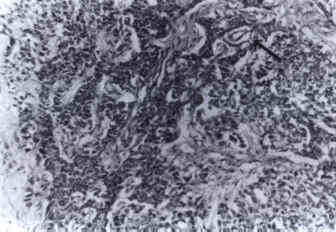
Fig. 1. CT scan showing the tumor mass (M) in the right hemithorax. Arterial blood gas analysis revealed mixed respiratory and metabolic acidosis and respiratory failure; hence the child was given ventilatory support. Later, he sustained a cardiac arrest and died after 16 hours of admission. At autopsy, there was a large, partly encapsulated anterior mediastinal mass that had infiltrated the upper and middle lobes of the right lung and was adherent to the right chest wall. It was soft, white and necrotic. Multiple histopathological sections studied showed a highly cellular tumor composed of round to oval cells with scant to moderate eosinophilic cytoplasm and large vesicular nuclei. These cells were disposed in varying patterns_solid sheets, trabeculae, glandular arrangement, microcystic areas and the formation of Schiller- Duval bodies (Fig. 2). Intracytoplasmic and extracellular hyaline, PAS positive and diastase resistant globules were also present. With these characteristic features and absence of other germ cell elements, a diagnosis of pure yolk sac tumor of the mediastinum was made.
Fig. 2. Yolk sac tumor showing trabecular arrangement of cells. Note perivascular formations (Schiller-Duval bodies), arrow (H&E, � 160). Discussion Pure yolk sac tumor or endodermal sinus tumor is a malignant germ cell tumor occurring mostly between one to five years of age at gonadal and extragonadal sites. Pure mediastinal yolk sac tumors are rare and most reported cases have been isolated case reports(3-7). Other unusual features are a male pre-ponderance and anterior mediastinal location of these tumors(3, 5-9). Our patient was also a male and the tumor occurred in the anterior mediastinum. As with other anterior mediastinal tumors, yolk sac tumors also present with cough, wheezing and respiratory distress. Our patient had presented with cough and breathlessness. As in our case, the time interval from the clinical onset to the diagnosis is short and the course is rapidly progressive(3,4). Elevation of alpha-fetoprotein (AFP) occurs with yolk sac tumors, since the fetal yolk sac is the source of physiological AFP in early embryogenesis. AFP levels should be measured at presentation and monitored during treatment and they are very useful in diagnosis and in evaluating the effectiveness of therapy(2-7). We could not document the same in our study because of the catastrophic course of the patient and due to the fact that the yolk sac tumor nature of the mass was not suspected. Yolk sac tumors are chemosensitive and various regimens are used for treatment like_PVB (Cisplatin, Vinblastine, Bleomycin), PEB (Cisplatin, Etoposide, Bleomycin) and JEB (Carboplatin, Etoposide, Bleomycin)(2). A total survival of 81% (at 5 years follow up) has been reported by the United Kingdom Children's Cancer Study Group(11). The yolk sac tumors are radioresistant and surgical excision is the treatment of choice(2). These tumors are chemo-sensitive; the response and disease control have improved dramatically with the advent of platinum based chemotherapy(2). Early diagnosis of a mediastinal mass is imperative by a CT scan. Histopathological confirmation should be done as early as possible as some of the tumors like the yolk sac tumor are chemosensitive and can show a dramatic response. Acknowledgement We thank our Dean, Dr. (Mrs.) P.M. Pai for permitting us to publish this case report. References 1. Birch JM, Marsden HB, Morris Jones PH, Pearson D, Blair V. Improvements in survival from childhood cancer: Results of a population based survey over 30 years. Br Med J 1988; 296: 1372-1376. 2. Castleberry RP, Cushing B, Perlman E, Hawkins EP. Germ cell tumors. In: Principles and Practice of Pediatric Oncology, 3rd edn. Eds. Pizzo PA, Poplack DG. Philadelphia, Lippincott-Raven Publishers, 1997; pp 921-945. 3. Sham JST, Fu KH, Chiu CSW, Lau WH, Choi PHK, Khin MA, et al. Experience with the management of primary endodermal sinus tumor of the mediastinum. Cancer 1989; 64: 756-761. 4. Shebib S, Sabbah RS, Sackey K, Akhtar M, Aur RJA. Endodermal sinus (yolk sac) tumor in infants and children. A clinical and pathologic study: An 11 year review. Am J Pediatr Hematol Oncol 1989; 11: 36-39. 5. Konishi T, Fujino S, Chino Y, Asada Y, Asakura S, Kato H, et al. Posterior mediastinal endodermal sinus (yolk sac) tumor in a female patient. Ann Thorac Surg 1994; 58: 244-245. 6. O' Sullivan P, Daneman A, Chan HSL, Smith C, Robey G, Fitz C, et al. Extragonadal endodermal sinus tumors in children: A review of 24 cases. Pediatr Radiol 1983; 13: 249-257. 7. Monig SP, Schmidt R, Krug B. Yolk sac tumor of the anterior mediastinum: The role of palliative surgery. Am Surg 1997; 63: 948-950. 8. Moran CA, Suster S, Koss MN. Primary germ cell tumors of the mediastinum: III. Yolk sac tumor, embryonal carcinoma, choriocarcinoma and combined nonteratomatous germ cell tumors of the mediastinum_A clinicopathologic and immunohistochemical study of 64 cases. Cancer 1997; 80: 699-707. 9. Moran CA, Suster S. Primary germ cell tumors of the mediastinum: I. Analysis of 322 cases with special emphasis on teratomatous lesions and a proposal for histopathologic classification and clinical staging. Cancer 1997; 80: 681-690. 10. Suster S, Moran CA, Dominguez - Malagon H, Quevedo - Blanco P. Germ cell tumors of the mediastinum and testis: A comparative immunohistochemical study of 120 cases. Hum Pathol 1998; 29: 737-742. 11. Mann JR, Pearson D, Barrett A, Raafat F, Barnes JM, Wallendszus KR. Results of the United Kingdom Children's Cancer Study Group's malignant germ cell tumor studies. Cancer 1989; 63: 1657-1667. |