|
|
Case Reports Indian Pediatrics 2000;37: 890-893 |
||
|
Persistent Hyperinsulinemic Hypoglycemia with Pyloric Stenosis |
||
From the Departments of Pediatrics and Pathology*, All India Institute of Medical Sciences, New Delhi 110029, India. Reprint requests: Dr. P.S.N. Menon, Genetic Unit, Department of Pediatrics, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110 029, India.
Manuscript Received: November 8, 1999; Persistent hyperinsulinemic hypoglycemia or Nesidioblastosis is an uncommon cause of neonatal hypoglycemia. Although most cases are sporadic, several authors(1,2) have des-cribed cases with an autosomal recessive inheritance. Nesidioblastosis has been asso-ciated with multiple endocrine adenomatosis and neuroblastoma(3). We hereby report the first case of nesidioblastosis and hypertrophic pyloric stenosis with presumed autosomal recessive inheritance.
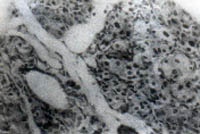
A male infant was born vaginally at 38 weeks of gestation with a birth weight of 4.2 kg. He was referred on day 3 of life with recurrent seizures. He was macrosomic, plethoric, and had hypertrichosis but no external malformations. There was no history of maternal diabetes and maternal HbA1c was normal. Investigations revealed hypoglycemia, which was intractable. He had repeated episodes of severe hypoglycemia and seizures even at glucose infusion rates of more than 15 mg/kg/min, requiring additional corticosteroids and glucagon to achieve euglycemia. He did not have ketonuria; his blood gases were normal. He had a serum insulin level of 114.1 pmol/L (15.9 mU/ml) during an episode of hypo-glycemia–at blood glucose of 1.1 mmol/L (20 mg/dl). The insulin to blood glucose ratio of 80 mU/mg was suggestive of hyperinsulinemia (normal <30). Ultrasonography revealed a normal pancreas. A diagnosis of persistent hyperinsulinemic hypoglycemia of infancy was made. A near total pancreatectomy was performed on day 14 of life. The histopathology of the pancreas revealed ductular insular complexes and large hyperchromatic beta cells with nuclear enlargement, suggestive of diffuse nesidioblastosis of the pancreas (Fig. 1). Postoperatively, blood glucose remained labile requiring frequent changes in the dose of glucose, insulin and glucagon to maintain euglycemia. He became euglycemic within 3 days and was discharged on the 14th post-operative day. Pancreatic enzyme supplements were administered at discharge. He was well till 1.5 months of age when he developed recurrent non-bilious vomiting. Examination revealed an abdominal lump characteristic of hypertrophic pyloric stenosis which was subsequently confirmed by barium studies (Fig. 2 ). The child underwent Ramstedt’s myotomy which relieved the symptoms. The parents were second cousins. Their first baby, born four years prior to the index case, was also macrosomic (4.8 kg), had hyper-insulinemia [serum insulin level of 502 pmol/L (70 mU/ml)], and uncontrolled hypoglycemia on glucose infusion rates of more than 15 mg/kg/min. The child’s clinical features and investigations (including a HIDA scan) were suggestive of extrahepatic biliary atresia. Unfortunately, the child died of septicemia before he could be operated upon.
Nesidioblastosis, a term first coined by Laidlaw in 1938, characterizes a condition with diffuse proliferation of disordered islet cells from pancreatic ductal cells. This term has now been replaced by persistent hyperinsulinemic hypoglycemia of infancy. Recent studies have identified mutations in various genes which can lead to this condition(4). The laboratory criteria for the diagnosis include the following: (i) inappropriately elevated plasma insulin concentration for the blood glucose value; (ii) an intravenous glucose infusion rate of more than 15 mg/kg/min to maintain a blood glucose level of more than 2 mmol/L (36 mg/dl); (iii) hypoketonemia; and (iv) a glycemic response to glucagon during hypoglycemia(5). The present case satisfied all the above mentioned criteria in addition to the histological features. Several cases of familial nesidioblastosis have been reported(1,2). The present case appears to have autosomal recessive inheritance due to normal but consanguineous parents and another affected sibling. The point of interest in this patient was the presence of congenital hypertrophic pyloric stenosis, an association, which has not been described earlier, to the best of our knowledge. One of the possible explana-tions for this association may be found in the common embryological development of the pancreas and the pylorus. The pancreatic tissue arises as two buds from the endoderm of the duodenum which divide later(6). The islets of Langerhans develop from the pancreatic parenchyma in the third month of the fetal life and the insulin secretion begins in the fifth(7). A maturational arrest thereafter is believed to cause nesidioblastosis. Although, the exact pathogenesis of hypertrophic pyloric stenosis is unclear, it is likely to be due to the failure of maturation or migration of ganglion cells to the pylorus during intrauterine life(8). The dis-ordered peristalsis results in the hypertrophy of the circular smooth muscles. Thus, an intrauterine insult, which could affect the maturation of both the ganglion cell and the islet cells, may explain the concurrence of the two conditions in the same patient. Similarly, neuroblastoma, which has been associated with nesidioblastosis(3), is considered to be due to an embryonic maturation arrest and prolifera-tion of primitive neuroectodermal cells. Apart from the embryological development defect accounting for this association, hypergastrinemia could be a linking factor. Hypergastrinemia and increased gastric acidity due to a genetically delivered supernormal parietal cell mass(9) may have a role in the pathogenesis of hypertrophic pyloric stenosis. Dysregulation of somatostatin production in nesidioblastosis or production of excessive gastrin by the pluripotent cells in nesidioblas-tosis may lead to a state of hypergastrinemia resulting in pyloric stenosis. However, in the present case, this mechanism would have limited role, as the child underwent near-total pancreactectomy on Day 14 of life. Interestingly, hypoglycemia with nesidio-blastosis and pyloric stenosis have been described separately in Smith Lemli Opitz syndrome(9,10). It would be interesting to study the histochemistry of the pancreatic tissue and serum hormone levels in the patients of nesidioblastosis in order to understand this enigmatic association. | ||
|