|
|
|
Indian Pediatr 2019;56: 698 |
 |
Double Aortic Arch Causing Prolonged Cough in a Child
|
|
Ira Shah 1
and Apurva Shrigiriwar2
1Pediatric TB Clinic, Department of
Pedeatric Infectious Diseases, BJ Wadia Hospital for Children, and
2Department of Pediatrics, Seth GS Medical College and KEM
Hospital, Mumbai, Maharashtra, India.
Email: 1
[email protected]
|
|
A 7-year-old girl presented in the pediatric tuberculosis clinic with
cough for 15 days. There was no fever or contact with an adult having
tuberculosis. She was tested in another hospital with a Mantoux test
that was positive, and was referred to us to start anti-tuberculous
therapy. On examination, weight was 20 kg with no abnormal findings.
Chest X-ray showed superior mediastinal widening. High resolution
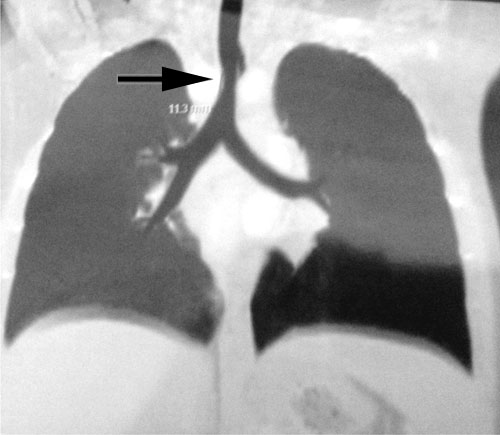
computed tomography (HRCT) of chest showed a double aortic arch forming
a vascular ring (the right arch measured 14 mm and the left arch
measured 12 mm) around the lower trachea and proximal thoracic esophagus
with the right arch indenting upon and causing mild narrowing of the
tracheal lumen (Fig. 1). She was subsequently referred to
the cardiac surgeon for further treatment.
(a) |
(b) |
|
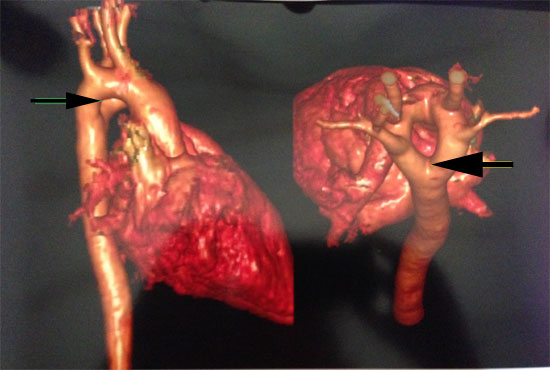
Fig. 1 (a) CT chest showing mild
narrowing of the tracheal lumen (arrow); 3D-reconstruction from
CT chest showing vascular ring around the lower trachea and
proximal thoracic esophagus (b).
|
Double arched aorta is a rare congenital
cardiovascular abnormality. Embryologically, one aortic branch arises
from each of the 4th branchial arches. Double aortic arch occurs as a
result of failure of involution of the right sided aortic branch which
persists beyond the embryonic stage. These two separate aortic arches
may join each other to form a vascular ring that can compress over the
trachea and esophagus manifesting as stridor, cough, wheezing and
recurrent pneumonias and/or with symptoms of esophageal compression
resulting in obstructive symptoms such as choking, regurgitation and
dysphagia [1]. All of these symptoms are non-specific; hence, these
patients can remain undiagnosed for many years. Chest X-ray may
show right sided aortic arch indenting the trachea and an increase in
paratracheal soft tissue thickness; sometimes bilateral aortic notches
can be seen at the level of aorta. A contrast enhanced computed
tomography (CT) or Magnetic resonance imaging is required to confirm the
diagnosis as well as aid in planning of surgical management, depending
on the type of arch dominance [2]. Management of these patients is
surgical with most patients having an excellent outcome and good
long-term prognosis [3].
References
1. Fenández-Tena A, Martínez-González C. Double
aortic arch diagnosed in a 44-year-old woman with recurring respiratory
infections. Respir Med Case Rep. 2017;20: 176-8.
2. Radiopedia. Double Aortic Arch. Available from:
https://radiopaedia.org/articles/double-aortic-arch: Accessed
Febuary 25, 2019.
3. Alsenaidi K, Gurofsky R, Karamlou T, Williams W,
MxCrindle. Management and outcomes of double aortic arch in 81 patients.
Pediatrics. 2006;118:e1336-41.
|
|
|
 |
|
