A 3-year-old girl presented to us for a rough aspect
of the trunk. Dermatologic examination showed multiple rough papules in
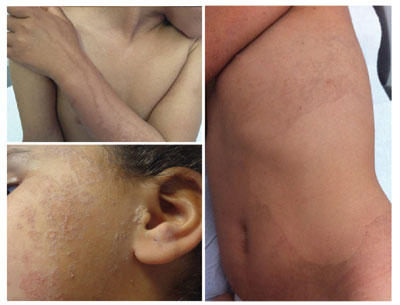
the upper and lower limbs (Fig. 1a), extending to the
trunk (Fig. 1b) and upper limbs with a linear arrangement,
and then to the face (Fig.1c).We also found a focal
palmoplantar keratoderma distributed in small islands. According to the
clinical aspect of the lesions, we suspected porokeratosis that was
confirmed by the skin biopsy. She was treated by acitretin (0.25
mg/kg/day) with good evolution within 3 months.
 |
|
Fig.1 (a) Multiple papules in the
upper limbs with a linear arrangement; (b) Multiple rough
papules in the trunk; and (c) Extended lesions to the trunk and
the face.
|
Porokeratotic eccrine ostial and dermal duct nevus
(PEODDN) is a rare variant of porokeratosis due to a mutation in GJB2
gene coding for the connexin 26 junction protein. PEODDN can present as
multiple hyperkeratotic or atrophic papules grouped on plaques with a
blashko linear arrangement. These lesions are mainly located at the
extremities and are frequently associated with a palmoplantar involvment.
Proximal involvement of the extremities, the trunk and the face, as seen
in this patient is very rare. The pathognomonic histological findings
are characterized by cornoid lamella located in relation of a dilated
sweat excretor canals and associated to vacuolated keratinocytes in the
epidermic invagination. Differential diagnoses include Linear
porokeratosis, linear lichen planus, linear verrucous epidermal nevus,
and linear Darier’s disease. PEODDN start at birth or in the early
childhood. Clinically it resembles a comedonal nevus, but it occurs on
the palms and soles where pilosebaceous follicles are normally absent.
Treatment options include dermocorticoids, topical calcipotriol,
cryotherapy, CO


