Cherubism is a rare genetic disorder with approximately 300 cases
reported worldwide. The disorder typically begins in children at ages of
2-7 years affecting males and females with equal frequency [1]. The
lesions usually first appear symmetrically in the angle of mandible;
rarely involvement of condyles and zygomatic arches has been reported.
Lesions are limited to the jaws, and in most cases begin to regress with
the onset of puberty. Respiratory problems due to backward displacement
of tongue or obliteration of the nasal airway may manifest as upper
airway obstruction. Extracranial involvement is extremely rare.
Biochemistry is usually normal in these patients [2].
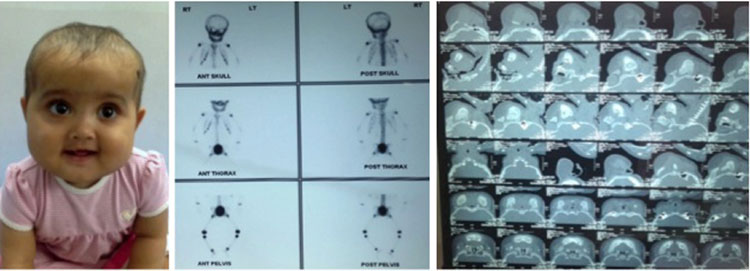
A 9-month-old girl presented with progressive
enlargement of the facial bones first noticed at 3 months of age. The
enlargement was gradual, involving the maxilla and the mandible
bilaterally initially (Fig. 1); followed by development of
palpable firm to hard lesions over affected bones without any pressure
symptoms. She was referred with a probable diagnosis of fibrous
dysplasia. CT scan revealed symmetrical enlargement of mandibles
involving the body, ramus, coronoid and condylar processes with loss of
normal trabecular pattern and ground glass opacity in involved bones (Fig.
1). Maxilla, sphenoid wings, body and pterygoid plates showed
similar changes. A bone scan revealed overgrowth of mandible with
increased uptake and no other significant bony abnormality. A biopsy was
advised but the parents refused for the same.
 |
|
Fig.1 (a) Typical faces of child showing fullness
of maxilla and mandible with upward slanting of eyes and the
sclera visible below the irises; (b) Bone scan
demonstrating increased uptake in the mandible and maxilla with
no other abnormality; (c) CT scan of the child
showing symmetrical enlargement of the mandibles.
|
Grading systems for cherubism have been suggested to
describe location and severity of lesions. There are no distinguishable
histological lesions specific for cherubism. The disease usually occurs
due to dominant mutations on SH3BP2 gene located on chromosome
4p16.3 [3,4]. The differential diagnoses include brown tumor of
hyperparathyroidism, giant cell lesions, fibrous dysplasia, aneurysmal
bone cyst and the hyperparathyroidism-jaw tumor syndrome.
Follow-up every 2 to 5 years is advisable after the
disease becomes quiescent. Surgical intervention is indicated when
aesthetic or functional concerns arise.
1. Jones WA. Familial multilocular cystic disease of
the jaws. Am J Cancer. 1933;17:946-50.
2. Kozakiewicz M, Perczynska-Partyka W, Kobos J.
Cherubism–clinical picture and treatment. Oral Dis. 2001;7:123-30.
3. Southgate J, Sarma U, Townend JV, Barron J,
Flanagan AM. Study of the cell biology and biochemistry of cherubism. J
Clin Pathol. 1998; 51:831-7.
4. Kalantar Motamedi MH. Treatment of cherubism with
locally aggressive behavior presenting in adulthood: Report of four
cases and a proposed new grading system. J Oral Maxillofac Surg.
1998;56:1336-42.


