|
|
|
Indian Pediatr 2015;52: 710-711 |
 |
CYP21A2 Gene Mutation in South Indian
Children with Congenital Adrenal Hyperplasia
|
|
*Ramaswamy Ganesh, Natarajan Suresh, Lalitha
Janakiraman and #Karnam
Ravikumar
Departments of Pediatrics and #Pediatric Endocrinology, Kanchi Kamakoti CHILDS Trust hospital and The CHILDS Trust Medical
Research Foundation, Chennai, Tamil Nadu, India.
Email:
ganeped79@rediffmail.com
|
|
Congenital adrenal hyperplasia (CAH) is an autosomal
recessive disorder; 21 hydroxylase deficiency is the most common cause
accounting for 95% of cases [1]. The extent of the enzyme impairment and
the clinical phenotype of the disease are determined by the severity of
the genetic defect in the CYP 21 gene [2]. We present here the
gene mutations seen in patients with CAH from Chennai, India, presenting
to the department of Pediatric endocrinology at Kanchi Kamakoti CHILDS
Trust Hospital, Chennai, India from August 2013 to July 2014. Children
diagnosed with classical congenital adrenal hyperplasia (salt-wasting
phenotype) based on the clinical features, serum electrolytes, 17
hydroxy progesterone levels and molecular genetic analysis, and followed
during the study period were included. Informed consent was obtained and
the study was approved by the Institutional ethics committee. Molecular
genetic testing of CYP21A2 gene was performed at All India
Institute of Medical Sciences, New Delhi.
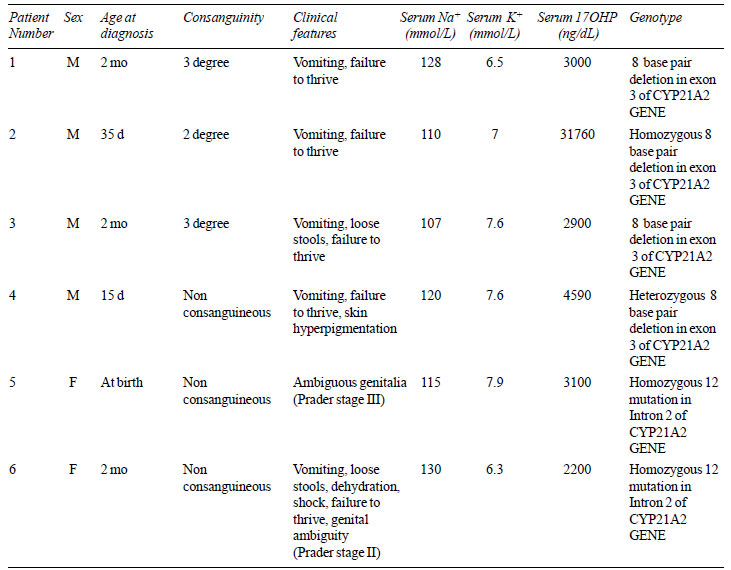
Abnormal genotype in CYP21A2 gene was detected
in 6 (4 boys) out of 10 children with CAH screened. Their clinico-laboratory
characteristics are shown in Table I. 8 base pair deletion
in exon 3 of CYP21A2 gene was the commonest mutation seen in 4
children, followed by 12 g deletion mutation in Intron 2 in the
remaining two. Mutation was not detected in four children. All children
were treated with hydrocortisone and fludrocortisone, and are doing well
at follow-up. Boys with CAH were diagnosed later than girls in our study
which is similar to an earlier study by Bajpai, et al.
[3], thus stressing the need to rigorously implement neonatal screening
of all children which will enhance the earlier diagnosis of less severe
forms of CAH, reduce the virilization in classical forms and promote
normal growth. Vomiting and failure to thrive were the most common
clinical presentation seen in both genders in our series, similar to an
earlier observation by Begum, et al. [4].
|
TABLE I Clinico – Laboratory Profile of
Children with CAH
|
 |
To date there are approximately 100 different
mutations reported in CYP 21 gene including deletions, point
mutations and insertions. Severe mutations are associated with classical
CAH whereas milder mutations are associated with non-classical CAH
[5,6]. Marumudi, et al. from New Delhi reported Intron 2 mutation
as the most common mutation in patients with CAH [7]. Mathur, et al.
[6] from New Delhi reported Ile173Asn followed by intron 2 splice and
Gln 319 stop mutations in children with classical CAH. In our series, 8
bp deletion in exon 3 of the CYP21A2 gene was the most common
(66.7%) followed by 12 g mutation in Intron 2 of the CYP21A2 gene
[IVS2-13A/C>G]. As complete sequencing of CYP21A2 gene is
expensive and is available only in select laboratories, knowledge of
common mutations prevalent in our population helps us to make a reliable
pre-, peri- and post-natal diagnosis, and also to offer genetic
counseling to the affected families.
References
1. Huynh T, McGown I, Cowley D, Nyunt O, Leong GM,
Harris M, et al. The clinical and biochemical spectrum of
congenital adrenal hyperplasia secondary to 21-hydroxylase deficiency.
Clin Biochem Rev. 2009;30:75-86.
2. Dolzan V, Stopar-Obreza M, Zerjav-Tansek M,
Breskvar K, Krzisnik C, Battelino T. Mutational spectrum of congenital
adrenal hyperplasia in Slovenian patients: A novel Ala15Thr mutation and
Pro30Leu within a larger gene conversion associated with a severe form
of the disease. Eur J Endocrinol. 2003;149:137-44.
3. Bajpai A, Kabra M, Menon PS. 21-Hydroxylase
deficiency: Clinical features, laboratory profile and pointers to
diagnosis in Indian children. Indian Pediatr. 2004;41:1226-32.
4. Begum JA, Sarker AK, Hoque M, Mamum MAA, Mobarak
MR, Biswas R, et al. Clinical profile of congenital adrenal
hyperplasia(CAH): A treatable disease. Dhaka Shishu (Children) Hospital
Journal. 2010;26:108-12.
5. Forest MG. Recent advances in the diagnosis and
management of congenital adrenal hyperplasia due to 21-hydroxylase
deficiency. Hum Reprod Update. 2004; 10:469-85.
6. Marumudi E, Sharma A, Kulshreshtha B, Khadgawat R,
Khurana ML, Ammini AC. Molecular genetic analysis of CYP21A2 gene in
patients with congenital adrenal hyperplasia. Indian J Endocrinol Metab.
2012;16:384-8.
7. Mathur R, Menon PS, Kabra M, Goyal RK, Verma IC.
Molecular characterization of mutations in Indian children with
congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency.
J Pediatr Endocrinol Metab. 2001;14:27-35.
|
|
|
 |
|
