|
|
|
Indian Pediatr 2015;52:
707-708 |
 |
Eosinophilic Gastroenteritis with Ascites
in a Child
|
|
Gui Ming,*Yan Bo and Yuan Li-ping
From Department of Pediatrics and *Medical
Technology, First Affiliated Hospital of Anhui Medical University,
Hefei, China.
Correspondence to: Dr. Yuan Li-ping, Department of
Pediatrics, The First Affiliated Hospital of Anhui Medical University,
Hefei, China 230022.
Email: [email protected]
Received: January 28, 2015;
Initial review: March 07, 2015;
Accepted: May 28, 2015.
|
|
Background: Asctites is rare in eosinophilic gastroenteritis.
Case characteristics: An 11-year-old boy who presented with
abdominal pain and ascites. Observation: Peripheral blood
examination revealed eosinophilia; serum IgE levels were raised. Biopsy
from gastric antrum revealed marked eosinophilic infiltration of mucosa.
Outcome: The child’s symptoms and clinical findings improved
after corticosteroids and anti-allergy treatment for 2 weeks.
Message: Children presenting with unexplained gastrointestinal
symptoms in the presence of ascites should be investigated for the
gastrointestinal tract allergic disease.
Keywords: Abdominal pain, Ascites; Endoscropy,
Eosinophilia.
|
|
Eosinophilic gastroenteritis is a rare disease of
unknown etiology, and is characterized by focal or diffuse eosinophilic
infiltration of the gastrointestinal tract. Eosinophilic
gastro-enteritis occurs over a wide age range – from infancy through the
seventh decade – but most commonly presents between second to fifth
decades of life [1]. In recent years, pediatric eosinophilic
gastroenteritis is increasingly being diagnosed. The clinical
presentation is variable, and its correct diagnosis mainly depends on
the histological findings. We present eosinophilic gastroenteritis in a
child with main presentation of ascites.
Case Report
An 11-year-old boy presented to us with abdominal
pain for 7 days. He had no history suggestive of tuberculosis and he was
not taking any medications. His medical history revealed no personal or
family history of gastrointestinal disorders, contact with tuberculosis
or history of allergies. On admission, the patient looked pale;
abdominal examination revealed periumbilical tenderness with ascites.
Rest of the systemic examination was normal. He had a white blood cell
count (WBC) 7.98×10 9/L with
eosinophil levels of 31%. His erythrocyte sedimentation rate, C-reactive
protein level, plasma amylase and urine amylase was normal; total IgE
level was 354 (normal <100) mIU/mL. Bone marrow examination showed
increased eosinophils in bone marrow. Stool examination for ova and
parasites was negative. The results of food allergies showed that he was
allergic to egg. Ultrasonography and computed tomography (CT) scan
showed abundant ascites. Ascitic fluid study revealed high total
leukocyte count (1005/ mL, 93% eosinophils), serum ascetic fluid to
albumin gradient (SAAG) 0.8 g/L. and lactic dehydrogenase (LDH) 608
IU/L. Esophagogastroduodenoscopy revealed hyperemia and edema, scattered
hyperemic patchy mucosal lesions and hemorrhagic spots in the gastric
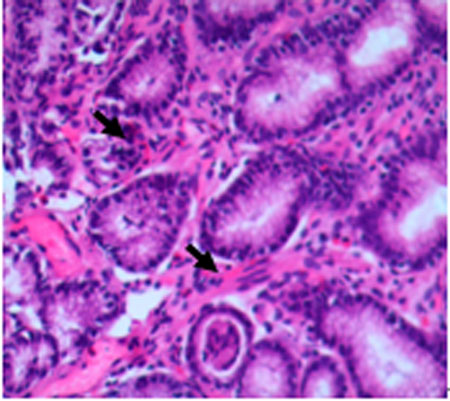
antrum and duodenum. Gastric antrum biopsy showed marked eosinophilic
infiltration in the mucosa (40/high power field) (Fig. 1).
 |
|
Fig. 1 History of antral biopsy
specimen demonstrating marked eosinophilic infiltrationin
hyperemic patchy mucosa. (See color image at website).
|
The patient was diagnosed as Eosinophilic
gastroenteritis and treated with prednisolone (20 mg/d) and cetrizine
(10mg) for two weeks. His symptoms improved rapidly, and the eosinophil
count normalized within 2 weeks. Prednisolone was tapered over 8 weeks
and cetirizine was used for about 4 months. The follow-up
eosophagogastro duodenoscopy after 5 months showed normal antral and
duodenal mucosa.
Discussion
Eosinophilic gastroenteritis is a rare disease of
unknown etiology and is defined as a gastrointestinal disorder of
undetermined cause characterized by infiltration of eosinophils in the
gastrointestinal tract. A strong history of allergy is usually prevalent
in these eosinophilic gastroenteritis patients, especially in the
pediatric population [1]. The present case satisfied criteria of
eosinophilic gastroenteritis [2]: (a) presence of
gastrointestinal symptoms; (b) biopsies demonstrating
eosinophilic infiltration of one or more areas of the gastrointestinal
tract, or characteristic radiological findings with peripheral
eosinophilia; and (c) no evidence of parasitic or
extra-intestinal disease.
The clinical manifestations of eosinophilic
gastroenteritis range from non-specific gastrointestinal complaints to
more specific symptoms such as protein-losing enteropathy, luminal
obstruction and eosinophilic ascites. In the past few years, a number of
cases of ascites as a clinical manifestation of eosinophilic
gastroenteritis in adults and children have been published [3-5]. There
is no standard treatment for eosinophilic gastroenteritis, but steroids,
anti-allergy treatment and allergy avoidance are often prescribed [6].
In severe cases refractory to medical management, and in those with
stenotic lesions, surgical resection of the affected areas may be
indicated. The child in present report responded satisfactorily to
medical management.
We conclude that eosinophilic gastroenteritis should
be suspected when unexplained gastrointestinal symptoms are present
along with peripheral esonophilia.
References
1. Liacouras CA, Furuta GT, Hirano I, Atkins D,
Attwood SE, Bonis PA, et al. Eosinophilic esophagitis: updated
consensus recommendations for children and adults. J Allergy Clin
Immunol. 2011;128:3-20.
2. Talley NJ, Shorter RG, Phillips SF, Zinsmeister
AR. Eosinophilic gastroenteritis: a clinicopathological study of
patients with disease of the mucosa, muscle layer, and subserosal
tissues. Gut. 1990;31:54-8.
3. Tas A, Celik H. An unusual cause of ascites in a
young patient. Turk J Gastroenterol. 2013;24:79-80.
4. Thielsen P, Rashid S, Klarskov LL. Eosinophilic
ascites is a rare presentation part of eosinophilic gastroenteritis.
Ugeskr Laeger. 2013;175:1577-8.
5. Gupta P, Singla R, Kumar S, Singh N, Nagpal P, Kar
P. Eosinophilic ascites, a rare presentation of eosinophilic
gastroenteritis. J Assoc Physicians India. 2012; 60:53-5.
6. Lucendo AJ, Arias A. Eosinophilic gastroenteritis: an update.
Expert Rev Gastroenterol Hepatol. 2012;6:591-601.
|
|
|
 |
|
