|
|
|
Indian Pediatr 2011;48: 643-644 |
 |
Nasal Foreign Body Presenting as Unilateral
Headache |
|
A Jain, M Shah and S Jain
From Department of Otorhinolaryngology and Head and Neck
Surgery, CU Shah Medical College and Hospital, Surendra Nagar, Gujarat,
India.
Correspondence to: Dr Anil Jain, 20, C- Block, Doctor’s
Quarters, CU Shah Medical College and Hospital, Dudhrej Road, Surendra
Nagar, Gujarat, India.
Received: February 12, 2010;
Initial review : March 11, 2010;
Accepted: May 3, 2010
|
We report a 6 year old female child, who presented with history of right
sided recurrent headache for four months. On diagnostic nasal endoscopy,
a metallic foreign body was seen impacted between superior turbinate,
middle turbinate and nasal septum which was removed using pediatric
nasal endoscope. Following removal, the symptom of unilateral headache
subsided. Possibility of a foreign body should always be ruled out while
evaluating a child with recurrent, unilateral headache.
Key words: Foreign body, Nose, Secondary headache, Unilateral
headache.
|
|
T
he commonest presentation of
unilateral nasal foreign body in pediatric age group is unilateral
recurrent rhinitis, unilateral purulent foul smelling rhinorrhea, and
unilateral epistaxis. They are usually reported early by patient or
relatives of patient to treating clinician and are managed
appropriately. Nasal foreign bodies includes button cells, stones,
beads, nuts, seeds, small erasers and toy parts. We report a child
who presented with unilateral headache and the diagnosed only after
months of impaction to have an atypical foreign body in nose.
Case Report
A 6-year old girl was referred from a general
practitioner with complain of right sided recurrent headache since
four months. She had no similar complain before that. Her visual
acuity and CNS examination was normal. On anterior rhinoscopic
examination, scanty, blood stained mucopus was seen in right nasal
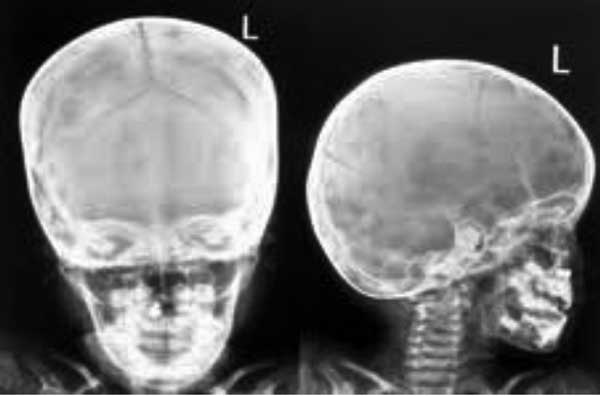
cavity. Roentogram of the skull demonstrated presence of a metallic
foreign body in right nasal cavity. Endoscopic examination was
suggestive of presence of some impacted, metallic foreign body in
right nasal cavity, between superior turbinate, middle turbinate and
nasal septum. There was no nasal septal deviation. Foreign body
(rusted metallic screw) was then removed under general anesthesia
using pediatric 0 degree nasal endoscope. After removal of foreign
body, patient was relieved of headache. Retrospectively patient gave
history that she had accidently introduced foreign body (screw) in
her right nostril while playing but she did not tell to any one at
that time due to fear and later on she forgot the incidence. Patient
is on regular follow up since one year and is well.
 |
|
Fig. 1 X-ray AP and lateral view of
Skull demonstrating the foreign body (metallic screw). |
Discussion
In this patient, even though, the foreign body was
there in the nasal cavity for four months and was causing recurrent
headache, yet it remained undiagnosed due to its unexpected
presentation.
The mechanism involved in headache due to foreign
body in nose can be explained by the fact that pressure exerted on
sensory nerves of adjacent lateral wall, can produce pain [1]. This
concept was first elaborated by Sluder, and the resultant condition
has been called ‘The anterior ethmoidal nerve syndrome’ [2]. In
addition to their direct neurological effects, reflex changes perhaps
may result from septal deformities, which affect nasopulmonary and
nasal reflexes.
Mcauliffe, et al. studied the sensitivity
of the nasal cavities and the paranasal sinuses using mainly faradic
stimulation and found that the lateral wall of the nasal cavity was
much more sensitive than the septum [3]. Clinical studies show that
the very severely impacted nasal septum can exert pressure on the
more sensitive structure of the lateral nasal wall and cause referred
trigeminal pain and chronic headache [4].
Thus, when a pediatric patient presents with such
a history, appropriate radiological evaluation should be carried out
and thorough nasal endoscopic examination has to be performed to
reach the correct diagnosis and appropriate management of patient.
Contributors: AJ: managed the case, reviewed
the literature and wrote the paper; MS: collected data; SJ:
critically reviewed. All authors helped in writing the manuscript.
Funding: None.
Competing interests: None stated.
References
1. David B. The nasal septum. In: Ian SM,
Bull TR, editors. Scott-Brown’s Otolaryngology. 6th ed. Oxford:
Butterworth – Heinemann publishers and distributers: 1997. P. 4:11.
2. Shalom, AS. The anterior ethmoid nerve
syndrome. J Laryngol Otol. 1963;77:315.
3. McAuliffe GW, Goodell H, Wolff HG. Experimental
studies on headache: Pain from the nasal and paranasal structures.
Research publication of the association for Research into Nervous and
Mental Diseases. 1943;23:185-206.
4. Schonsted MU, Stoksted P, Christensen PH, Koch-HN.
Chronic headache related to nasal obstruction. J Laryngol Otol.
1986;100:65-170.
|
|
|
 |
|
