|
|
Case Reports Indian Pediatrics 2007;44:615-617 |
||
|
Pulmonary Sarcoidosis Masquerading as Tuberculosis |
||
|
Meenu Singh From the Pediatric Pulmonology unit, Advanced Pediatric Center, Post Graduate Institute of Medical Education and Research, Chandigarh, India. Correspondence to: Dr Meenu Singh, Additional Professor of Pediatrics, Advanced Pediatric Center, PGIMER, Chandigarh 160 012, India. E-mail: [email protected]
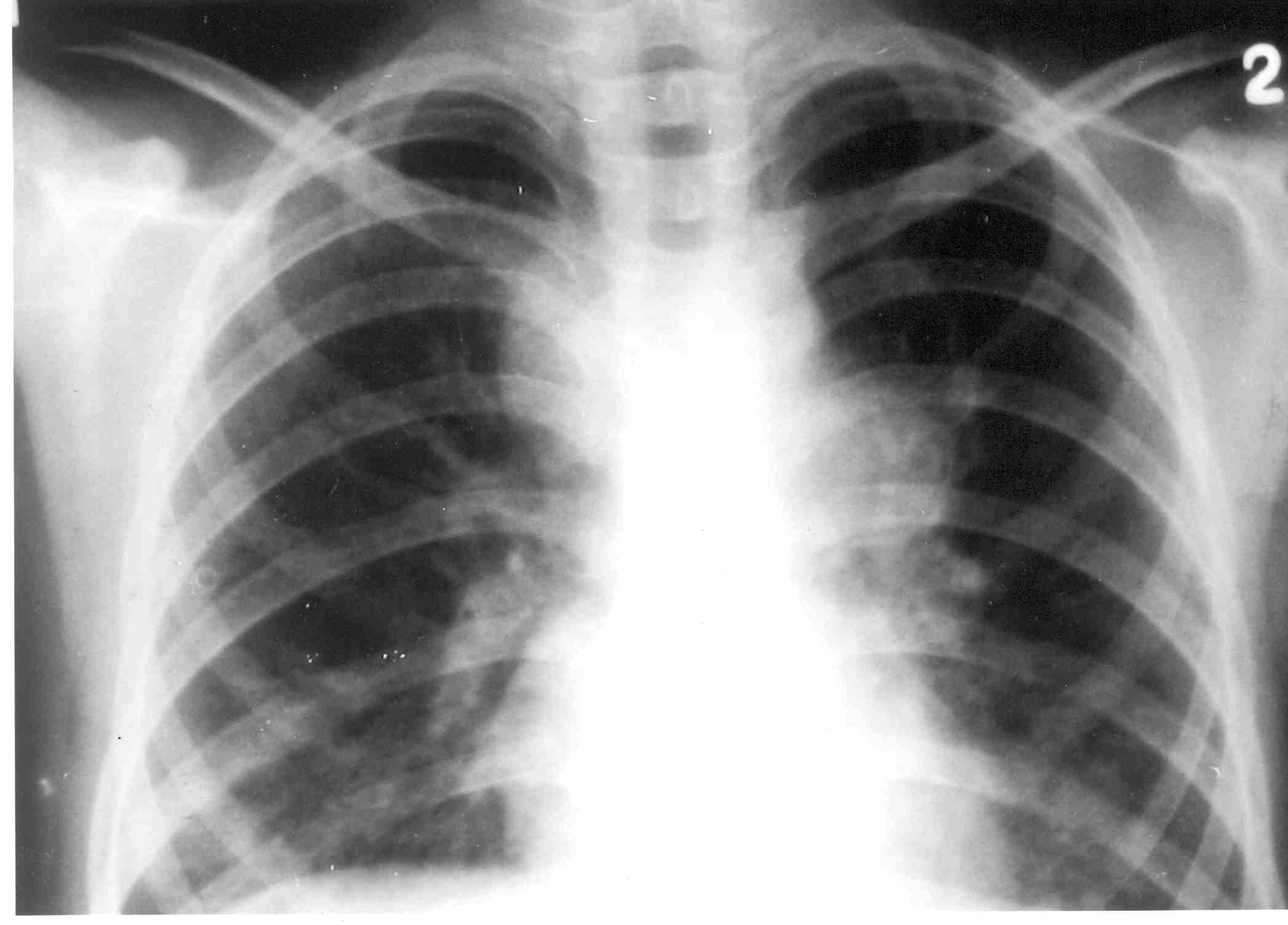
Abstract: Key words: Pulmonary Sarcoidosis. Sarcoidosis is a chronic, multisystem, granulomatous disorder which occurs with an incidence of 0.22-0.27 per 100,000 children per year(1). In developing countries like India, sarcoidosis is underreported probably due to lack of awareness and the presence of other more prevalent granulomatous diseases, especially tuberculosis. The diagnosis of sarcoidosis is established when a compatible clinical and radiographic picture is supported by histologic evidence of noncaseating granulomas in affected tissues as well as exclusion of other granulomatous diseases (e.g., tuberculosis, histoplasmosis, blastomycosis). Literature search revealed 12 cases of pediatric sarcoidosis in India. Nine of them were reported from general wards of hospitals while the remaining 3 were from pediatric unit of AIIMS, New Delhi(2,3). Case Report An 11-year-old girl presented with history of occasional non productive cough and intermittent low grade fever for 2 months. Few cases of pulmonary tuberculosis were reported recently from school in which she was studying. She was not exposed to organic dust, drugs or recurrent aspiration. On examination she had poor weight gain and pallor. There was no clubbing, skin rash, joint involvement, lymphadenopathy or organomegaly. Chest examination revealed bilateral fine inspiratory crepitations. Her hemoglobin was 10.4 g/dL and erythrocyte sedimentation rate was 30 mm. Mantoux test showed a skin reaction of 10 × 10 mm. Gastric aspirate for acid fast bacillus was negative on three occassions. Sputum had not shown any acid fast bacillus, bacteria or fungus. Chest X-ray (Fig. 1) showed bilateral lower zone consolidation with reticulonodular shadows with prominent hilar lymphadenopathy. In view of strong epidemiological history, chronic pulmonary symptoms and radiological abnormalities, possibility of pulmonary tuberculosis was considered. She was started on RHZE(Isoniazid – 5 mg/kg, Rifampicin – 10 mg/kg, Ethambutol – 20 mg/kg and Pyrazinamide – 25 mg/kg) as per IAP protocol(4). There was neither clinical nor radiological improvement even after 6 months of anti tubercular therapy including a trial against multi drug resistant tuberculosis. She was also evaluated for cystic fibrosis. Sweat chloride was 30 mEq/L. Pulmonary function tests showed predominant restrictive pattern with decreased FEV1 [1.2 L/S 60% of expected] FVC [1.3L/S 66% of expected] and decreased single-breath carbon monoxide diffusing capacity (DLCO 18.6 mL/min/mm Hg). High resolution computer tomography (Fig. 2) revealed para tracheal, subcarinal lymphadenopathy, reticulonodular infiltrates in lower lobes and mild interlobular septal thickening consistent with interstitial lung disease. Echo-cardiography was normal. Serum was negative for ANA, ANCA and HIV. Serum calcium was normal. Angiotensin converting enzyme levels were elevated [55.8 U/L (normal range 8-52 U/L)]. Possibility of sarcoidosis was considered and open lung biopsy (4 sites) was performed. Histopathology showed noncaseating granulomas consistent with sarcoidosis. She was started on oral prednisolone 2 mg/kg/day for 4 weeks followed by slow tapering. She had shown a significant improvement in her symptoms. Other systemic evaluation for sarcoidosis including eyes was normal. Within 4 weeks of steroid treatment, lung function had improved [FEV1 (85%), FVC 70% of expected)] and radiographic appearances showed improvement, with significant resolution of parenchymal nodular infiltrates.
Discussion Sarcoidosis is characterized by the formation of nonnecrotizing epitheloid cell granulomas as a result of underlying immune dysregulation and typically shows multiorgan involvement. The initial clinical presentation of sarcoidosis is variable, depending on the organ systems involved, but in most pediatric cases includes fever, weight loss, fatigue, bone and joint pain, anemia, hepato-splenomegaly and lymphadenopathy. In children younger than 5 years, the disease is characterized by involvement of skin, eyes and joints, whereas in older children involvement of lungs, lymph nodes and eyes predominate(5,6). Though initially we considered tuberculosis in view of hilar lymphadenopathy and strong epidemiologic history, progressive symptoms, negative bacteriological studies for tuberculosis, poor response to ATT, and predominant restrictive pulmonary function tests prompted us to investigate for other causes like interstitial lung disease (primary and secondary). Bilateral hilar lymph node enlargement and symmetrical pulmonary infiltrates helped us in suspecting sarcoidosis as a cause of her pulmonary symptoms which was later supported by elevated ACE levels and lung biopsy. Sarcoidosis constitutes 2% of interstitial lung disease(7). In the vast majority, cough and pulmonary symptomatology are not the primary features. Approximately 50% of children with sarcoidosis have impaired lung function tests with a restrictive pattern. Reduced lung function with an obstructive pattern has been reported in approximately 15% of children which was present in index case(7). Chest radiographs are abnormal in more than 90% of patients with sarcoidosis. The most characteristic finding on chest radiograph is bilateral hilar lymph node enlargement, (seen in 50% to 85% of cases) and central, bilateral reticular or reticulonodular opacities. Our index case qualifies for stage 2 according to radiological classification criteria. High-resolution CT scan of index case revealed peribronchial thickening, subpleural nodularity and traction bronchiectasis which are diagnostic of sarcoidosis(9).Other tests that may provide supportive evidence for sarcoidosis include increased acute phase reactants and serum ACE level. Hypercalcemia is seen in up to 30% of cases(6-8). Our index case had become is asymptomatic and shown significant improvement of lung function tests in follow up and is on low dose steroids(10). Diagnosis is delayed in our country due to lack of awareness, presence of more prevalent diseases like tuberculosis and lack of investigative facilities especially for isolated pulmonary sarcoidosis(2,3). One should have a high index of suspicion for diagnosis of this condition when a child presents with chronic pulmonary symptoms with typical radiological findings. After excluding other common causes, one should proceed with lung biopsy to confirm it. Contributors: KK and MS were involved in patient management and review of literature; MS shall act as guarantor. Funding: None. Competing interests: None stated. | ||
|
References | ||
|
![]()