|
|
Case Reports Indian Pediatrics 2007;44:611-612 |
||||
|
‘Screw’ - Appendicitis |
||||
|
Ram Samujh
Appendicitis due to foreign bodies is rare and carries an incidence of 0.005%(1-3).Stones, bullets, airgun pellets, pins etc. have been described in the appendix. Metallic screw can become lodged in the appendix leading to appendicitis or even gangrene/perforation in more severe cases. We present a 4 -year-old Saudi boy who was found to have a metallic screw within the appendix. The screw was visualized on plain X-ray abdomen and on fluoroscopy but its presence within the appendiceal lumen was confirmed only on surgical exploration. Case Report A four-year-old Saudi boy presented to emergency room with 24 hours of abdominal pain in right lower quadrant. There was no history of vomiting or diarrhea. There was no clear history of foreign body ingestion. However; there was history of recurrent abdominal pain for last 4 months. On examination, the child was active and afebrile. There was no pallor or cyanosis. Vital signs were stable. Examination of the abdomen revealed mild tenderness in right iliac fossa. There was no guarding/ rigidity or rebound tenderness. Rectal examination was unremarkable. Other systemic examination was normal. On investigations, hemoglobin was 12.9 g/dL; TLC was 16,900/mm3 with 85% polymorphs. Serum electrolytes, blood urea and serum creatinine were normal. Plain roentgenogram of the abdomen showed one metallic screw in right lower abdomen (Fig. 1). Ultrasonography of abdomen could not detect the foreign body and reported as normal study. Fluoroscopy revealed a metallic foreign body-screw in right iliac fossa but it was not sure whether it was in appendix or embedded in the cecal wall as the foreign body was fixed in position.
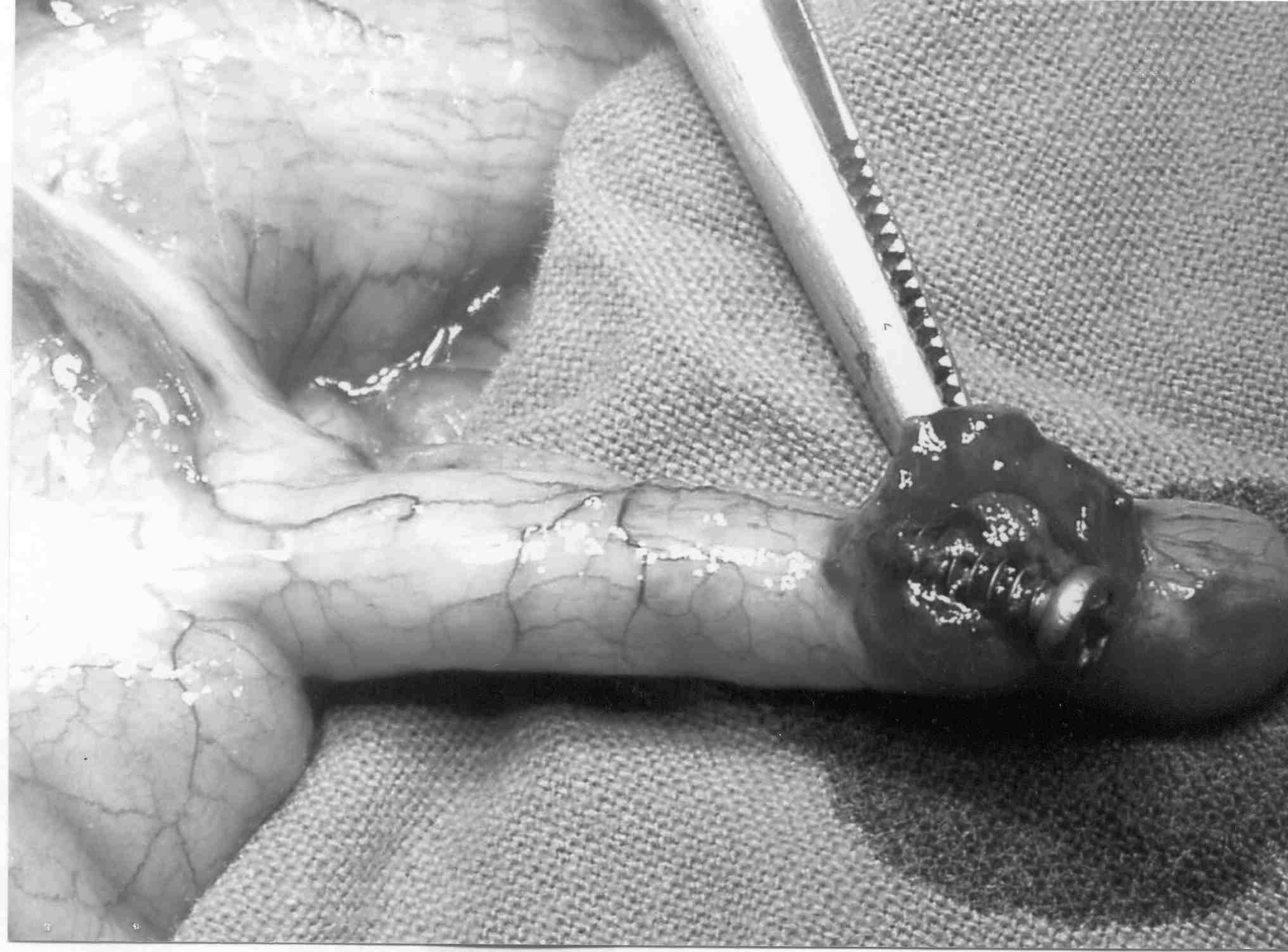
The abdomen was explored by a right lower transverse incision. The appendix was found to be mildly inflamed with a screw in its lumen embedded at the distal end of the appendix (Fig. 2). The histopathological examination of the appendix showed features of early acute appendicitis. Postappendicectomy, patient improved and was discharged on 5th postoperative day. The patient was asymptomatic on one year follow-up.
Discussion To best of our knowledge, this is the first case of foreign body appendicitis caused by screw in a child. Needles(I,2), shotgun pellets(4), bird shots(5), hazelnut(6), canine hair (70), sand and stones(8) have been reported as a cause of foreign body appendicitis in children. In a series of 217 cases of appendiceal foreign bodies reviewed by Balch & Silver(3), pins were found to be most common. Ingested foreign bodies may have an uneventful course or it can cause perforation of the bowel including appendix. Most of the foreign bodies pass through the gastrointestinal tract within a week without causing any disease manifestation(9). The reported incidence of bowel perforation is less than 1% especially with sharp, thin, stiff, pointed and long objects(10). Foreign body appendicitis can be diagnosed by a careful history of foreign body ingestion, clinical examination, and plain X-ray abdomen showing foreign body in a static position on serial radio-graphs and lastly, laparoscopy can be used for diagnostic as well as therapeutic purposes. Contributors: RS conception & design, acquisition of data, final approval of the manuscript; KM drafting of manuscript and analysis; IK critical revision of data, analysis; AM conception of data, analysis & interpretation of data Funding: None. Competing interests: None stated.
| ||||
|
References | ||||
|
![]()