|
|
Letters to the Editor Indian Pediatrics 2006; 43:744-745 |
|||
|
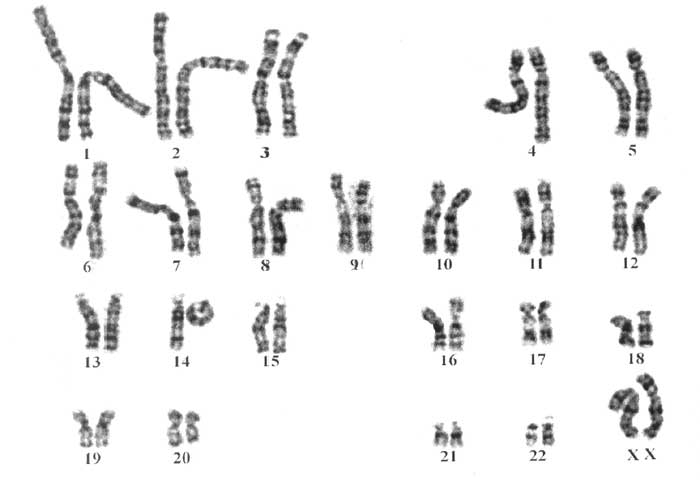
Ring Chromosome 14 with Epilepsy and Development Delay |
|||
|
The abnormality r(14) is a rare cytogenetic disorder with characteristic features and episode of uncontrolled seizures(1). Most of these features are also found in patients with linear terminal deletion of chromosome 14, except for seizures and retinal abnormalities. Schiade, et al.(2) carried a study to search for the cause of seizures in six patients with r(14) and three patients with deletion of distal 14q. It had indicated that it is unlikely to be a specific deleted locus in 14q32.3 that predisposes r(14) patients to seizure and retinal pigmentation. Similar observation was made by van Karnebeek, et al,(3) where child had linear deletion and deletion due to r(14), having same break point in 14q and had seizures and retinal pigmentation. Several hypotheses are put forward to explain these, including mitotic instability of ring chromosome, a telomere position effect in ring chromosomes in which 14p telomere silences nearby genes on the q arm and close dependant genes involved in seizures and retinal pigmentation located on the short arm of chromosome 14(3,4). The characteristic morphologic features of r(14) are thought to be contributed by the terminal deletion of chromosome 14 [q32.3-qter)(5). Though drug resistant epilepsy has been observed in some study, our patient compliance with the monotherapy for seizures, absence of brain atrophy and moderate microcephaly could be attributable to the age of presentation and absence of #14 monosomy. This explains why proband is not resistant to antiepilectic therapy. In such cases, parents carry the risk of 1-2% in subsequent pregnancy if the r(14) is of de-novo origin. However the risk increases significantly [~40%] if mother carry ring chromosome while heterozygote male is usually infertile. To conclude, chromosome analysis appears necessary for a child with epilepsy, developmental delay and ophthalmic involvement. Parental study will ensure the counseling for the recurrent risk in such abnormalities. Frenny J. Sheth,
|
![]()