|
|
Original Article Indian Pediatrics 2005; 42:773-781 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Additional Markers to Refine the World Health Organization Algorithm for Diagnosis of Pneumonia | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
A.V. Castro, C.M. Nascimento-Carvalho, F. Ney-Oliveira,
*C.A. Araújo-Neto, *S.C.S. Andrade,
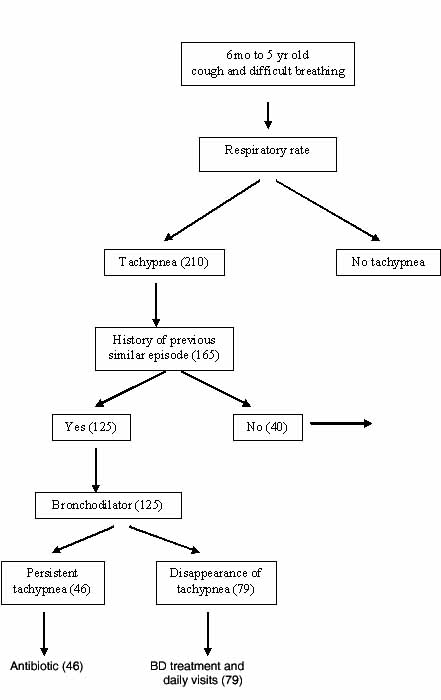
Childhood pneumonia remains a relevant and well discussed subject because of its high mortality in developing countries. It is estimated that 13 million children aged less than 5 years die worldwide, annually(1); among them about 4 million children die from pneumonia in developing countries(2). Because of such a high mortality, the World Health Organization (WHO) developed the Program for the Control of Respiratory Infections in the 1980’s(3), which was included as a component of the Integrated Management of Childhood Illness (IMCI) strategy in the mid 1990’s(4). This strategy included the utilization of simple signs and symptoms with high sensitivity and specificity to be adopted at first level health facilities by paramedical personnel(4). Using this algorithm, pneumonia is diagnosed by the presence of tachypnea defined as: respiratory rates ≥60 breaths/minute among children aged < 2 months, ≥50 breaths/ minute among children aged 2-11 months and ≥40 breaths/minute among children aged 12-59 months. Because mortality due to pneumonia in developing countries is attributable mainly to pyogenic bacterial etiology, IMCI strategy recommends the use of antibiotics when the child presents tachypnea as defined previously(4). Despite the proven benefit of this program(5), there has been some concern about the specificity of the WHO pneumonia algorithm and IMCI leading to the un-necessary use of antibiotics in regions with high prevalence of wheezing illness(6). In this context, it is also important to consider that asthma and other wheezing illnesses do occur and they can be diagnosed in children who present with cough and difficult breathing, and they can be treated with only bronchodilators (BD) without the need of antibiotics(7). The health consequences of asthma-like symptoms in children without the diagnosis of asthma are substantial(8).This study was designed to evaluate the potential use of fever, chest indrawing and the effect of bronchodialator response in children with cough and tachypnea and history of previous respiratory distress as tools to exclude the diagnosis of pneumonia, and thus to refine the use of antibiotics. Subjects and Methods This study was performed in the pediatric emergency room (ER) of an urban tertiary hospital in Salvador, Northeast Brazil, from March, 2003 to June, 2004. The local peak season for respiratory illness includes months from April to September. Sample size was calculated by using Statsdirect software in order to compare paired proportions; in the study, each patient was compared with himself, before and after the use of BD, whenever there was history of previous episode of respiratory distress. It was estimated that the use of BD was underused by 35%(7); 0.1 was the correlation coefficient of failure between the paired tests, power was 80% and alpha was 5%; so minimal sample size was 124 patients. Entry criteria were children aged between 6 and 59 months attending the ER because of cough and difficult breathing for less than 5 days, presenting tachypnea as defined by WHO guidelines. Written informed consent was obtained from parents or legal guardians before recruitment. Children with severe malnutrition (defined as weight for age under - 2SD by using the National Center for Health Statistics pattern)(9), grunting and underlying chronic illness except asthma were excluded. The study was approved by the institutional review board of the hospital and by the Ethics Committee and Research of the Faculty of Medicine of Federal University of Bahia. Data collection was based on a questionnaire which included demographic and clinical findings to be filled out by the duty pediatrician who were trained before the beginning of this investigation. A pilot study was conducted to test all procedures involved in data collection and to standardize the collection of data to be performed by pediatricians and radiologists. Several symptoms and signs were recorded: history of fever, refusal of feeds, cyanosis, alertness, nasal flaring, runny nose; axillary temperature was recorded for 3 minutes and fever was defined as axillary temperature ³37.5ºC; respiratory rate was counted by observing the movement of chest and abdomen for 60 seconds in a quiet and awake child; chest indrawing was sought by observing the inward movement of the bony structures of lower chest wall; audible wheeze was searched for during 30 seconds prior to auscultation with stethoscope; breathing and other sounds, such as crackles and wheeze, were searched during auscultation. A history of a previous episode of cough and difficult breathing was recorded for each eligible patient. Whenever, the answer was yes, treatment with BD was started. BD therapy was done by use of a wet nebulizer during a one hour period (3 doses of beta2-agonist, 0.1mg/kg/dose, each 20 minutes). After the initial BD challenge, the subjects were evaluated with particular attention to respiratory rate and improvement in difficult breathing. This was recorded in the questionnaire and then a chest X-ray was performed. Diagnostic Definitions Clinical diagnosis of pneumonia was performed by the pediatrician before reading the chest X-ray if the respiratory frequency had not reduced under the cutoff limit for respective age stratum. For the purpose of this study, only radiological diagnosis of pneumonia by both radiologists was considered. Agreement on interpretation of infiltrates between 2 pediatric radiologists was necessary for evaluation in the study. The radiologists were not given clinical information and considered only 3 radiological patterns: (i) normal, (ii) presence of pulmonary infiltrates (reduced pulmonary view), or (iii) pulmonary hyperinflation without pulmonary infiltrate, based on WHO standards and definitions applied for epidemiological studies(10). Bronchospasm was diagnosed if there was wheeze, absence of pulmonary infiltration on chest X-ray and rapid improvement (reduction of respiratory rate below cutoff limit for each age) after BD therapy. Co-existence of bronchospasm and pneumonia was defined if the respiratory rate decreased and there was concomitant pulmonary infiltrate on X-ray. Therefore, the gold standard for diagnosis of pneumonia was presence of pulmonary infiltrate described by both radiologists. Data Analysis Statistical analysis were performed by using EpiInfo v.6 and Statistical Package for the Social Sciences (SPSS 9.0). Differences in proportions were assessed by Pearson Chi Square or Fisher’s exact test as appropriate. Sensitivity, specificity, positive and negative predictive values and likelihood ratios with respective 95% confidence interval were calculated to assess the resolution of tachypnea after BD use on ruling out pneumonia. Stratified analysis considering the presence of fever or chest indrawing was performed. The statistical tests were two tailed, with a significance level of 0.05. Results Of 210 recruited children, 28 cases (13.3%) were excluded because of poor quality of chest X-ray. Of the remaining 182 children, 165 had concordance of radio-graphic opinion regarding infiltrates, there-fore, became the study group for this evaluation. Forty patients had no previous history of respiratory distress. 125 children (75.8%) had a history of respiratory distress and therefore received BD challenge to evaluate the response in tachypnea. These 125 were the subject of the sub-group analysis regarding the role of BD in diagnostic decision making in determining the existence or not of pneumonia. The median age was 22 months (mean 25.1 ± 14.5 months) and 75.8% were ³1 year of age. There were 58.8% males. Table I shows the clinical characteristics of the patients. No other condition like dehydration, acidosis or severe anemia was recognized as cause for fast breathing in the studied group. Previous respiratory distress was reported in 65.0% of children aged less than 1 year and in 79.2% of older ones. The analysis was not stratified by age because the number of children younger than 12 months was not appropriate for statistical analysis. Pneumonia was radio-logically diagnosed in 15.8% (26/165) of the children, in 2/40 (5.0%) without history of previous respiratory distress, and in 24/125 (19.2%) children with a history of previous respiratory distress and who received BD. Both patients with pulmonary infiltrate with-out history of previous respiratory distress were female, aged 36 or 29 months old, with respiratory frequency registered as 52 or 56, respectively. Among 125 children with history of previous respiratory distress, 14 (11.2%) had only pneumonia, 101 (80.8%) had only bronchospasm and 10 (8.0%) had pneumonia and bronchospasm (Fig. 1). Table I Clinical Characteristics of 165 Children with Cough and Rapid Breathing.
Persistent tachypnea (14/24, 58.3%) after BD use was associated with presence of pulmonary infiltrates, whereas tachypnea persisted in 32/101 (31.7%) children without infiltrates (P = 0.02). Assessment for presence of pulmonary infiltrate and persistent tachypnea demonstrated sensitivity 58.3% (95% CI 36.9 - 77.2), specificity 68.3 (95% CI 58.2 - 77.0), predictive value positive 30.4% (95% CI 18.2 - 45.9), predictive value negative 87.3% (95% CI 77.5 - 93.4), likelihood ratio positive 1.84 and likelihood ratio negative 0.6 (Table II). Table II Results of the Algorithm used in this Study and of the Radiological Reading.
Table III shows the stratified analysis of the BD response (disappearance or persistence of tachypnea) according to whether there was also fever or chest indrawing in patients with a history of previous respiratory distress. The data indicates that fever was not a reliable indicator as only 8/24 (33.3%) patients with pneumonia had fever; however, in the absence of fever, 56.3% of these had persistent tachypnea after BD challenge (P = 0.03). Chest indrawing was common in all patients, and not associated with the presence of pneumonia. However, in the presence of chest indrawing, there was more likely to be absence of a tachypnea response to BD (P = 0.02). Table III Association of bronchodilator responsive or persistent tachypnea with fever or chest indrawing with pulmonary infiltrate in 125 children with previous history of respiratory distress.
In summary, this study indicates that absence of a response in tachypnea to BD challenge may be useful in children without fever or with chest indrawing, in identifying those with pneumonia as the cause of cough and tachypnea. Discussion At the time of conception of WHO guidelines for case management of childhood pneumonia in early 1980s, pneumonia was assumed to be the predominant condition presenting with fast breathing(3). Up to this moment, enough data have been accumulated to highlight the increasing prevalence and severity of asthma globally, another condition presenting with fast breathing(11). It has been demonstrated a considerable overlap in clinical presentation of acute asthma and pneumonia and under-treatment with BD and overuse of antibiotics(7,11). It is also necessary to emphasize that asthma related fatalities do occur and can be prevented by an accurate diagnosis and early institution of appropriate therapy including BD(12). It had been previously demonstrated that in Salvador, Northeast Brazil, 44.7% of children with pneumonia presented wheezing and asthma was reported in 53.8% of them with preexisting illness(13). Data from the International Study of Asthma and Allergies in Childhood demonstrated that Brazil was the eighth country in the frequency of wheezing and Salvador is the Brazilian city with the highest prevalence(14). These data may explain the high frequency of children with a history of previous similar attack (65.0% and 77.5% of children aged <1 year and ³1 year, respectively) in this study. It is noteworthy the low frequency of pneumonia cases (15.8%), which is in accordance with the great importance of asthma as a cause of respiratory distress in the region where this study was conducted. In a previous study, in India, a small number of pneumonia alone (<10%) was diagnosed when BD was used to refine the prescription of antibiotics in children with cough and difficult breathing(7). The inclusion of cough as a mandatory criterion in the entry point, as suggested by Sachdev, et al.(7), certainly explains the absence of nonrespiratory illnesses as cause of tachypnea from the patients studied in this investigation. This study demonstrated association between persistent tachypnea after BD therapy in children with history of previous respiratory distress and presence of pulmonary infiltrate (58.3% vs 31.7%, P = 0.02) (Table II). So, if one considers persistence of tachypnea among those children as a clinical diagnosis of pneumonia, then it is associated with radiological diagnosis of pneumonia. By employing the algorithm used in this study and presented in Fig .1, 87.3% (95% CI 77.5 - 93.4) of patients did not receive unnecessary antibiotics and 41.7% of patients with pulmonary infiltrate would not have received antibiotics, on clinical basis accessible to primary health care workers in the first evaluation. The response to BD in children with history of previous respiratory distress could reduce the use of antibiotics mainly in regions with high prevalence of wheezing illness(6). Considering the antibiotic use as the key driver of resistance(15) and the fact that many countries have expressed growing concern about the problem of antimicrobial resistance(16), it is suggested to evaluate in further investigations, in other regions of the world, the introduction of the question "Has the patient ever had cough with respiratory distress before?" in the case management for children presenting with cough and tachypnea. For those with resolution of tachypnea after BD therapy, it is suggested daily visits by paramedical personnel in order to guarantee that children with pneumonia be identified and treated. Table III shows the statistical association between presence of fever or chest indrawing and presence of pulmonary infiltrate. Although Taylor, et al. have given evidence on the predictive value of tachypnea considering WHO guidelines in spite of fever(17), this study emphasizes the recommendation of treating fever before counting the respiratory rate of children with cough, difficult breathing and history of previous respiratory distress. The modifier effect of presence of chest indrawing is in accordance with previous studies where children with tachypnea and chest indrawing presented greater predictive value positive for pneumonia than children with only tachypnea(18). Limitations in this study must be considered. There was a small number of patients aged <1 year and stratified analysis according with age was not possible. The frequency of pneumonia and of other conditions that present with cough and difficult breathing are different in different age strata. Therefore, it is highly desirable to study the algorithm presented in Fig. 1 in children aged < and ³1 year. The results of this investigation may not be generalized to children living in regions with different prevalence of asthma. It is important to emphasize the use of coincident chest X-ray reading by 2 blinded independent pediatric radiologists in the analysis presented herein. Presence of pulmonary infiltrate remains the gold standard for the diagnosis of pneumonia(19). The present study provides evidence that the use of BD in children with cough, tachypnea and history of previous respiratory distress may differentiate children with pneumonia from children with broncho-spasm. Acknowledgements We acknowledge Prof. Anibal Silvany Neto for his technical assistance in the statistical analysis. Contributors: AVC designed the study, analyzed, collected and interpreted data, drafted the manu-script.CMN designed the study, analyzed data, revised and analyzed critically the manuscript and contributed in all phases of the study. FN recorded data, had participation in statistic analysis and discussion.CAA and SCSA interpreted the radio-graphs and analyzed critically to improve the radiological questions. LLSL and POL were clinical investigators, collected data and helped to review this manuscript. Funding: Nil. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()