From the Departments of Pediatric Surgery and
Histopathology*, Advanced Pediatric Center, Postgraduate Institute of
Medical Education and Research, Chandigarh, India 160 012.
Correspondence to: Dr. Ram Samujh, Postgraduate
Institute of Medical Education and Research, Chandigarh, India 160 012.
E-mail: rsamujh@yahoo.com
Manuscript received: June 19, 2003; Initial review
completed: July 29, 2003; Revision accepted: January 20, 2004.
Abstract:
Rhabdomyoma is a rare benign tumour, majority arising from the
cardiac muscle. Seventy to 90% of extra cardiac rhabdomyomas are found
in the head and neck region, usually within the upper aero digestive
tract. We report a case of rhabdomyoma of anterior neck in a neonate.
Although rhabdomyomas of posterior neck have been reported, those
reported in anterior triangle are infrequent. The lesion has not
recurred one year after complete excision. There are no similar
reports in Indian literature.
Kew words: Newborn, Rhabdomyoma.
Introduction
The term rhabdomyoma was introduced by Zenker (1864)
to indicate a benign tumour showing skeletal muscle cell with varying
degree of differentiation and maturity(1). It was considered as a
general diagnostic term for tumor as granular cell myoblastoma, alveolar
soft tissue sarcoma, sarcoma botryoides, embryonal rhabdomyosarcoma,
teratoma and mesenchymomas(2). Rhabdomyomas are currently defined as
benign neoplasm of striated muscle tissue, consisting usually of
polygonal frequently vacuolated glycogen containing cells with a fine
granular deeply acidophilic cytoplasm resembling myofibril in cut
section(3).
Most of the extracardiac rhabdomyomas in head and
neck region in children are usually in posterior auricular region and
pharynx. Anterior neck is an infrequent site. We report a case of extra
cardiac rhabdomyoma of anterior neck in an infant.
Case Report
One-month-old female child presented with a swelling
in the left submandibular region since birth. There was no redness or
discharge and no feeding or respiratory difficulty noted. The general
physical examination was unremarkable. The systemic examination did not
reveal any abnormality. Local examination revealed a 8 × 6 cm swelling
in left submandibular region, having bosselated surface, firm
consistency, non tender, bimanually palpable and extending into the
floor of mouth. The overlying skin was normal. There was no redness,
scar or sinus or lymphadenopathy. X-ray soft tissue neck revealed
a soft tissue mass with no calcification. Ultrasonography showed a solid
lesion with heterogeneous and hyperechoic areas and no calcification.
Fine needle aspiration cytology suggested a spindle cell tumor. NCCT
head showed a septate cystic homogenous mass with extension superiorly
behind the ramus of mandible, inferiorly till thoracic inlet, medially
to the left para pharyngeal space displacing larynx and left carotid
vessels and posteriorly reaching upto the border of sternocleidomastoid
muscle. Local excision of tumor was done which revealed a well-defined
solid tumor with cystic areas deep to omohyoid muscle in left sub
mandibular region with no local infiltration. Histopathology of the
resected tumor showed features of fetal rhabdomyoma. On
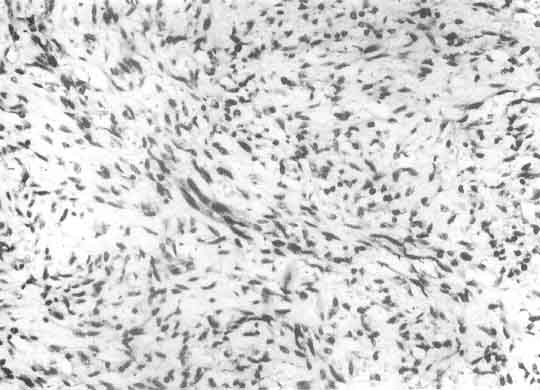
histopathological examination, the tumor was composed of oval to spindle
cells with vasicular nuclei. In most areas there was abundant
intercellular myxoid material with few inflammatory cells (Fig.1).
Few cellular areas with fascicular arrangement were seen. There was no
pleomorphism or mitotic activity. Occasional strap cells with abundant
eosinophilic cytoplasm were seen which showed cross striations by PTAH
stain (Fig. 2), confirming skeletal muscle differentiation. The
tumor cells were positive for desmin on immunohistochemistry.
 |
 |
|
Fig. 1. Photomicrograph of the tumor to show spindle cells
in a loose Myxoid background (H. & E. × 140). |
Fig. 2. Photomicrograph to show cross striations (arrow) in
the tumor cell (PTAH × 1360). |
Discussion
Rhabdomyomas are rare benign neoplasms of skeletal
muscle cells found more frequently in the myocardium than in the
striated muscles. The rare extra cardiac rhabdomyomas are true neoplasm
and 70% occur in head and neck region. They are subdivided into adult,
fetal and genital histological subtypes(4,5). The adult type of
rhabdomyomas occur exclusively in the head and neck region. These are
soft, coarsely lobulated tan to grey and well-circumscribed tumors
ranging in size from 0.5 to 6.0 cm. Age of the patients range from 16 to
82 years (mean age 52 years). There is a marked male predominance of
almost 5:1. A clonel balanced translocation has been found in Chromosome
15 & 17 in the head and neck rhabdomyoma(6). Majority of them require
local excision with few local recurrence. Each recurrence is usually
treated by local excision.
Fetal rhabdomyomas are benign tumors with skeletal
muscle differentiation that have a propensity to occur in head and
region. They are composed of elongated spindle shaped skeletal muscle
elements in varying stages of differentiation. They are subdivided into
two histological sub types "classic" immature histology and others with
more prominent rhabdomyoblastic maturation "intermediate" histology(7).
However, several tumors show overlapping features between classic and
intermediate groups suggesting that these are more likely a single group
with a spectrum of rhabdomyoblastic differentiation(7).
Fetal rhabdomyomas usually present as solitary mass
within the soft tissue or the mucosal areas of head and neck. The may
also present with hoarseness, dysphasia or respiratory distress. The
most common sites are post auricular region, pre auricular region, or
face, followed by nasopharynx and oral cavity. The differential
diagnosis includes rhabdomyosarcomas (spindle cell variant) and benign
hamartomatous lesions, such as neuro-muscular hamartomas and
rhabdomyomatous measenchymal hamartomas of the skin(8,9). Distinction
from spindle cell variant of rhabdomyosarcoma and other embryonal
rhabdomyosarcomas may be difficult. Unlike rhabdomyosarcomas, which has
infiltrative margins and invades normal tissues, fetal rhabdomyomas are
well circumscribed and do not invade and destroy adjacent soft tissue.
Histologically foetal rhabdomyomas rarely show areas of necrosis, and
unlike rhabdomyosarcomas they lack hypercellularity, a "cambium layer"
typical of botryoid rhabdomyosarmas, nuclear atypia, abnormally
distributed chromatin and absent or low mitotic activity(10).
The subgroups of extra cardiac rhabdomyomas can
further be characterized by immunocyto-chemical studies staining the
myoglobin desmin vimentin muscle specific actin. Desmin is the most
reliable marker for cells with skeletal or smooth muscle differentiation
as it is present in both primitive and mature cells. Vimentin is present
in primitive cells and myoglobin is present in mature cells(11).
The possibility of fetal rhabdomyoma should always be
considered in differential diagnosis of a cervical swelling especially
in a neonate.
Contributors: RS, AD reviewed literature and
prepared the manuscript, KJ made the diagnosis on histopathology; KLNR
managed the patient and will act as guarantor.
Funding: None.
Competing interests: None stated.
