|
|
Images in Clinical Practice Indian Pediatrics 2003; 40:790-791 |
||||
|
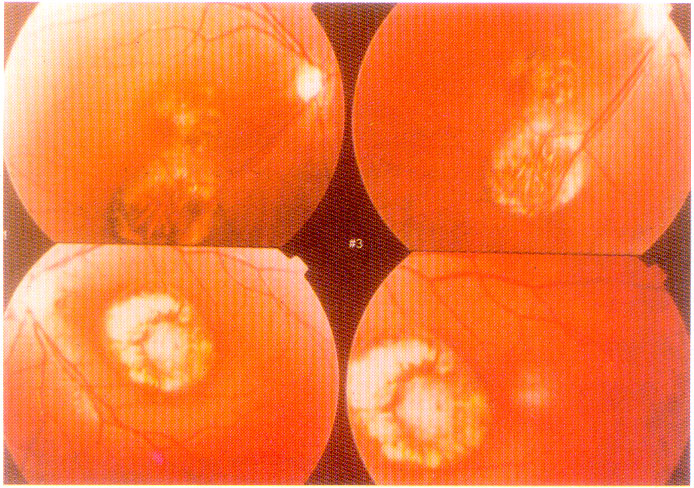
Chorioretinitis in Congenital Toxoplasmosis |
||||
|
A 12-year-old boy presented with recurrent attacks of afebrile generalized seizure since 5-years of age. His mother had an uneventful antenatal, natal and post-natal period. His growth and development was normal. He had normal facies, normal head size, strabismus, no CNS abnormality. His IQ was 72. His visual acuity in left eye was 2/60 and 3/60 in the right eye. Ophthalmoscopic examination revealed bilateral central chorioretinitis involving macula (Fig. 1). CT scan of brain revealed focal dot like hyperdensity in right posterior parietal region (Fig. 2). Toxoplasma ABS EIA results were within normal limits (Toxoplasma IgG AB-2.66; reference range <7.00 IU/ml and Toxoplasma IgM ABS-0.29; reference range <1.00 IU/ml). A Diagnosis of congenital toxoplasmosis was made based on the clinical triad of convulsions, cerebral calcification, and chorioretinitis.
Congenital toxoplasmosis results from transplacental transmission of T. gondii infection. Most of the infection are subclinical with few cases of clinical congenital toxo-plasmosis. The congenitally infected infants who are normal in the perinatal period will almost have ocular involvement in later life. Chrioretinitis is the most frequent abnormality in patients with congenital infection being present in about 75-80% of cases. It is bilateral in 85% of affected individuals. In the fundus there are bilateral and frequently multiple chorioretinal lesions, the macular area being particularly involved. The whole thickness of the retina and choroid is destroyed in a necrotizing inflammation, so that a punched out, heavily pigmented scar remains. It is probable that many cases labeled congenital colobomata due to intra-uterine inflammation have this etiology. The differential diagnosis includes congenital colobomatous defect and other inflammatory lesions due to Herpes simplex virus, Cytomegtalovirus, Treponema pallidum, Mycobacterium tuberculosis or vasculitis. Sumana Datta (Kanjilal),
|
![]()