|
|
Case Reports Indian Pediatrics 2002; 39:392-395 |
||
|
Hydrops Fetalis and Extralobar Lung Sequestration |
||
|
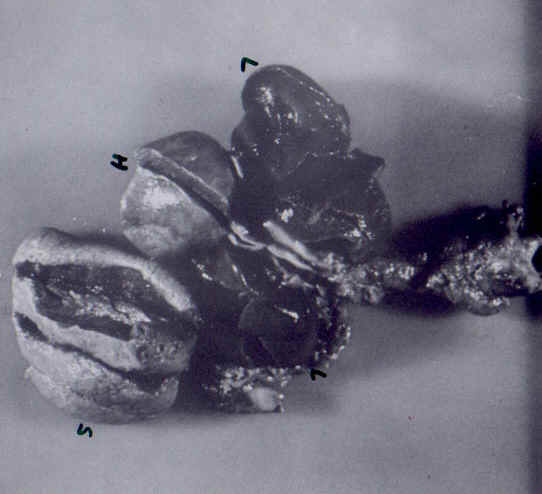
Extralobar lung sequestration (ELS) is a congenital cystic lesion comprising of non-functional lung tissue that does not communicate with the normal tracheo-bronchial tree. The lesion receives its arterial blood supply from an aberrant branch of the aorta (rather than pulmonary artery) and is drained by pulmonary veins. ELS is usually asymptomatic and presentation as hydrops fetalis is extremely rare. We present one such case of left-sided extralobar pulmonary sequestration with hydrops, bilateral pleural effusion, ipsilateral pulmonary hypoplasia and respiratory distress syndrome (RDS). Case Report A 33-year-old third gravida woman had her first antenatal ultrasound (US) at 32 weeks gestation. Sonography revealed bilateral pleural effusion, mediastinal shift to right and moderate ascites. There was no evidence of polyhydramnios or any other malformation. Fetal echocardiography was normal. She tested sero-negative for VDRL and TORCH infection. Blood group was A positive with negative indirect Coomb’s test. Glucose tolerance test was in the normal range. Family history was non-contributory. In view of hydrops and fetal distress, the woman was taken up for caesarian section at 34 weeks and a 2.9 kg male baby was delivered. On examination he was found to be a term baby. He required bag and tube ventilation. Bilateral thoracocentesis was done for poor chest expansion and 50 ml and 5 ml straw colored fluid was aspirated from left and right sides, respectively. Apgar scores were 4 at 1 minute, 5 at 5 minutes and 5 at 10 minutes, respectively. Umbilical arterial sample revealed a pH of 7.2, PaCO2 of 33 mmHg, PaO2 of 19 mmHg, HCO3 of 13.1 mmHg and ABE of- 15.3. The baby was put on the ventilator for poor respiratory effort. The initial ventilator settings were PIP 38, PEEP 5 and FiO2 1.0. X-ray chest and US chest revealed left sided pleural effusion. Left thoracostomy was done soon after birth for pleural effusion. The baby required a thoracostomy on the right side for pneumothorax at 2 hours of age. At 8 hours, he developed differential cyanosis with right upper limb saturation of 55% with PaO2 of 50 mmHg and a lower limb saturation of 25% with a PaO2 of 10 mmHg. Both femorals were well palpable and there was no difference in upper and lower limb blood pressures. A diagnosis of persistent pulmonary hypertension was considered and high frequency ventilation and alkalinization with sodium bicarbonate was tried, but it did not help. The baby expired at 17 hours of age. His VDRL and TORCH titers were negative. Karyotype was normal. Autopsy was performed with parental consent. It revealed a left-sided loose, spongy, cystic mass, deriving its arterial supply from the descending aorta. It weighed 17.5 grams. This was the extralobar pulmonary sequestration from the left lung. There was an associated hypoplasia of left lung, which weighed 5.5 grams (Fig. 1). The weight of right lung was 14..5 grams, against a normal mean weight of 17-19 grams at 37-38 weeks gestation. Histopathology of the mass revealed dilated sub pleural lymphatics, considered characteristic of ELS. Histopathology of lungs revealed hyaline membranes in the alveoli (secondary RDS). Hyaline membranes suggestive of RDS were absent in the sequestrated lung although the alveoli and alveolar ducts were atelectatic. Changes suggestive of persistent pulmonary hyper-tension were absent. A preductal coarctation was also present, which migh have been responsible for the differential cyanosis in the baby. There were no other associated anomalies.
Fig. 1. Autopsy specimen showing extralobar lung sequestration. L = lung, H = heart, S = sequestration. Discussion Extralobar lung sequenstration (ELS) is frequently asymptomatic and diagnosed accidently due to co-incident illness. Rarely, it may present in the neonatal period with respiratory distress or in later infancy with frequent chest infections and non-resolving pneumonia. Presentation in the fetal period with hydrops fetalis and pleural effusion is extremely rare. The first case of ELS associated with hydrops was published by Romero et al. in 1981(1). Review of literature revealed 24 cases of ELS with hydrops and pleural effusion(2). This is the first case report of ELS with hydrops from India. With the widespread use of antenatal ultrasound (US), ELS is likely to be diagnosed more frequently. Demonstration of aberrant lung tissue (solid and echogenic) receiving systemic blood supply is pathognomonic for the prenatal diagnosis of pulmonary sequestation(3). In our case the diagnosis of ELS was missed antenatally probably due to a significant pleural effusion and a lack of experience in diagnosing this condition. This has been described previously in the cases reported by Evans(4). ELS associated with pleural effusion and hydrops has a poor prognosis and considered to be a harbinger of fetal death if left untreated(3). It has been postulated that pleural effusion may occur due to venous and lymphatic obstruction secondary to the torsion of the vascular pedicle supplying the ELS. Alternatively the effusion may develop due to a large gradient between the systemic artery and the pulmonary veins. Large persistent effusions may result in hydrops due to compression of the vena cava. Only two cases of ELS with hydrops have been reported to undergo spontaneous resolution(5). Of the 24 cases of ELS with hydrops and pleural effusion reported till now, 9 have succumbed and 15 have survived(3). The prognosis of ELS with hydrops is likely to improve with the advent of in-utero surgery. The current recommendation for treatment of fetal hydrothorax is the placement of a pleuroamniotic shunt (PAS) and if unavailable, serial thoracocentesis may be tried. In our country where fetal therapy is still a distant dream, a different approach as adopted earlier may be a viable option(4,5). This approach involves continuation of pregnancy with delivery at around 32-34 weeks, aggressive postnatal management of hydrops and semi-elective resection of the ELS in the postnatal period. In our patient, the diagnosis of ELS was established post-mortem and no active therapy towards treatment of ELS could be attempted. Contributors: AU and RA were responsible for the neonatal work up and CS conducted the autopsy. AU drafted the manuscript and RA critically reviewed the manuscript. RA would act as the guarantor for the paper. Funding: None. Competing interests: None stated.
| ||
| References | ||
|
![]()