|
|
|
Indian Pediatr 2021;58:338-344 |
 |
Catalytic Support for
Improving Clinical Care in Special Newborn Care Units (SNCU)
Through Composite SNCU Quality of Care Index (SQCI)
|
|
Harish Kumar, 1 Rajat
Khanna,2 Varun Alwadhi,3
Ashfaq Ahmed Bhat,2 Sutapa B
Neogi,4
Pradeep Choudhry2, Prasant
Kumar Saboth1 and Ajay Khera5
From 1VRIDDHI, IPE Global Ltd.; 2Norway India Partnership Initiative;
3Department of Pediatrics, Kalawati Saran Children’s Hospital;
4International Institute of Health Management Research; and
5Ministry of
Health and Family Welfare, Government of India; New Delhi, India.
Correspondence to: Dr Ashfaq Ahmed Bhat, Norway India Partnership
Initiative, New Delhi, India.
Email: [email protected]
Received: April 30, 2020;
Initial review: June 29, 2020;
Accepted: November 17, 2020.
|
Objective: To develop a composite index that
serves as a proxy marker of quality of clinical service and pilot test
its use in 11 special neonatal care units (SNCUs) across two states in
India.
Design: Secondary data from SNCU webportal.
Settings: Special new-born care units in
Rajasthan and Orissa.
Intervention: We developed a composite SNCU
Quality of care Index (SQCI) based on seven indices from SNCU online
database. These included rational admission index, index for rational
use of antibiotics, inborn birth asphyxia index, index for mortality in
normal weight babies, low birth weight admission index, low birth weight
survival index, and optimal bed utilization index.
Outcome: Based on the SQCI score, the performance
of SNCUs was labelled as good (SQCI 0.71- 1.0), satisfactory (SQCI 0.4-
0.7) or unsatisfactory (SQCI <0.4).
Results: The mean difference in SQCI between
Jan-Mar 2016 and 2017 was 0.20 (95% CI 0.13- 0.28; P<0.001).
Similar results were obtained for rational admission index, rational use
of antibiotics, mortality in normal weight babies, low birth weight
survival and optimal bed utilization. A significant improvement in the
overall composite score was noted in Odisha (Mean difference 0.22, 95%
CI 0.11-0.33, P=0.003) and Rajasthan (Mean difference 0.17, 95%
CI 0.05- 0.3, P=0.002). Conclusion: QI approach using SQCI
tool is a useful and replicable intervention. Preliminary results show
that it does lead to strengthening of implementation of the programs at
SNCUs based on the comprehensive scores generated as part of routine
system.
Keywords: District hospital, Health programs, Health system,
Quality improvement.
|
|
I
ndia has experienced a rapid expansion of
Facility Based Newborn Care (FBNC) at various levels in the
health system in the last decade. The services provided at each
level is a product of infrastructure, availability of skilled
manpower, capacity of the institution and referral mechanisms
available. The facilities have been classified as newborn care
corners (NBCC) at every point of child birth, newborn
stabilization units (NBSUs) at first referral units (FRUs) and
special newborn care units (SNCUs) at district hospitals [1].
Ministry of Health and Family Welfare (MoHFW), Government of
India (GoI) under National Health Mission (NHM) has ensured
functional SNCUs, in most of the District Hospitals in the
country and has plans to further strengthen these units [2,3].
The SNCUs are equipped to manage small and
sick neonates except those who need mechanical ventilation and
surgical care. These units have admission and discharge criteria
for optimal utilization of services and bed strength and
services [4]. SNCUs have resulted in improvement in case
fatality among newborns admitted to hospitals [5]. However,
there are challenges in infrastructure, manpower and care
practices [6]. There is a need to assess the performance of
SNCUs with respect to quality of patient care, organization and
process to support improvement and enhance accountability
[5,7-9].
Experiences from QI programs on FBNC are also
limited [10-13]. Reports have uncovered the insuffi-ciencies of
data management systems to monitor key indicators. To address
this gap, GoI with support from UNICEF and Norway India
Partnership Initiative (NIPI) established a web-based data
management and tracking system, ‘SNCU online’ in the year 2011,
to be used across all the SNCUs in India. Between April, 2016
and March, 2017, SNCU online was functional in 571 SNCUs across
27 states with data available for more than 700,000 infants.
Measurement of quality of clinical services
rendered in the SNCUs is essential for feedback and improvement.
The objective of this study was to develop a composite index
that serves as a proxy marker of quality of clinical service and
pilot test its use in SNCUs in India.
METHODS
This study was conducted in two stages/phases
viz., development of a composite index (SNCU Quality of Care
Index or SQCI), and pilot testing the tool for feasibility and
applicability in SNCUs.
Development of SQCI: A team consisting of
six experts from national and state NIPI team developed a
comprehensive tool drawing relevant indicators from SNCU online
web portal. The process, spanning over a four month period,
involved field visits and observations by pediatricians and
statisticians. While defining the indices, due considerations
were given on whether those were in accordance with global norms
and standards for measuring quality of clinical care,
user-friendliness, access to available data, ability to do
self-assessment, and utility to Government for providing timely
feedback. The focus was to have a dynamic model that could
assess the optimal utilization of services, identify gaps in
skills and clinical practices that influence the case fatality
in every SNCU. For each of these objectives, most appropriate
indicators were identified and put into a statistical model to
arrive at a composite index. This was then piloted in one SNCU
to test for its reliability, feasibility and usefulness in
public health settings.
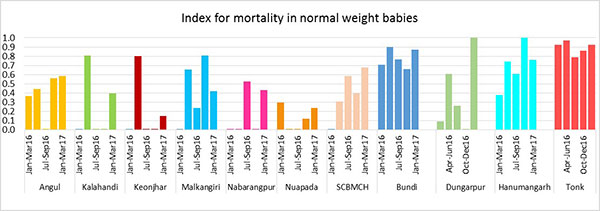
Initially, six indices were selected for
SQCI, which also included an index on total deaths in the SNCU.
Since this index was not able to measure the specific quality of
care issues in the SNCU, it was replaced with mortality in
normal weight babies ( ³2500
gram). Additionally, one more indicator was added on inborn
birth asphyxia index, to measure whether asphyxia was managed
adequately in the labour room, and its subsequent load and
implication on SNCUs in terms of bed occupation.
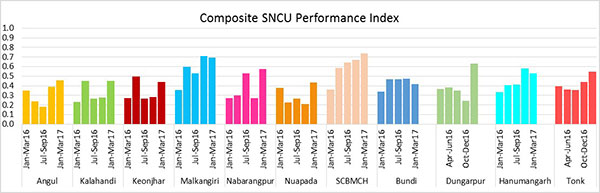
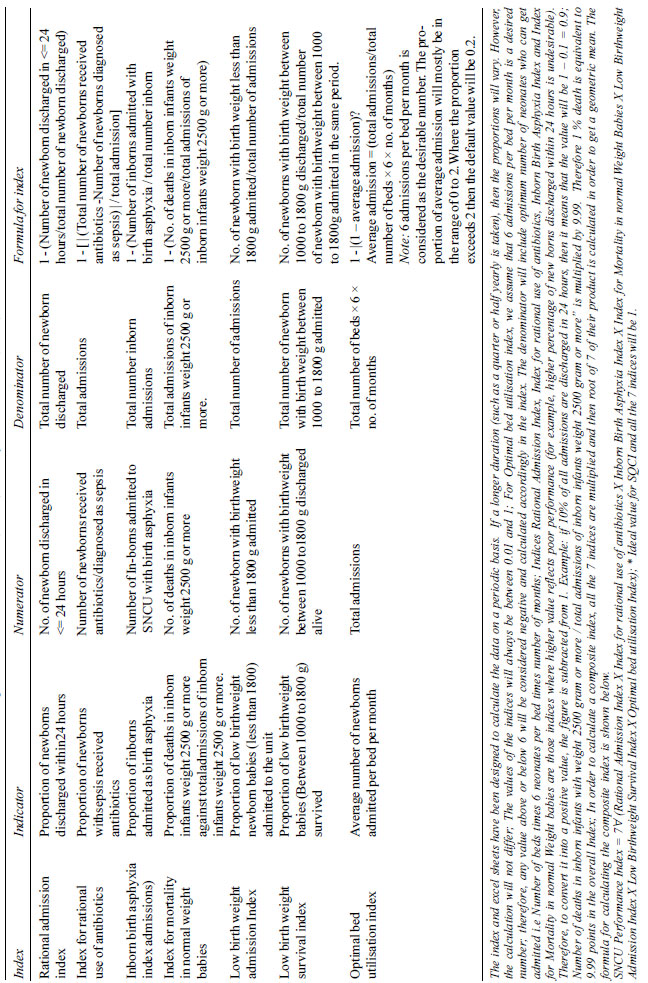
SQCI is a composite index of seven indices,
each having a range from 0.01 to 1 (Table I and
Web
Table I): rational admission index, index for rational use
of antibiotics, inborn birth asphyxia index, index for mortality
in normal weight babies, low birth weight admission index, low
birth weight survival index, optimal bed utilization index.
Since the indices are comparing different items and each item
has multiple properties, we have taken the geometric mean to
calculate the final score. Based on the SQCI score, the
performance of SNCUs was assessed as a Likert scale and labelled
as good (SQCI 0.71- 1.0), satisfactory (SQCI 0.4- 0.7) and
unsatisfactory (SQCI <0.4) [14].
|
Table I Special Newborn Care Unit
(SNCU) Quality of Care Index (SQCI) Calculations
|
 |
Data collection: The SQCI tool was used
in the states of Rajasthan and Odisha. All the parameters were
retrieved in each quarter of the year, recorded in a predesigned
excel database and SQCI score calculated by the program team.
The indices were calculated for every month and then compiled
for each quarter of the year. Each index was color coded (red
for unsatisfactory, yellow for satisfactory and green for good)
for better understanding. No additional data were collected for
the purpose of the study.
Overall feedback, with particular emphasis on
the two worst indicators, was provided to the districts. This
facilitated improvement in the performance of the SNCUs.
Permission and approvals were obtained from
concerned authorities (MoHFW, State governments) for retrieval
and analysis of data from SNCU database. Anonymity and rights of
patients and doctors were respected and therefore we did not
consider individual level data in our analysis.
The data for SQCI computation was taken from
an ongoing program and hence no ethical issues were involved.
Since this was a program evaluation based on routinely collected
data, no additional data was collected.
Data of five quarters starting from Jan- Mar
2016 to Jan- Mar 2017 were compared to assess the change in the
quality of services. Paired t test was done to explore
the statistical significance of the difference over a period of
one year (from Jan-Mar, 2016 to Jan-Mar, 2017).
RESULTS
We present the results as composite scores
aggregated from the SNCUs for the two states. In the pilot
phase, data from 11 SNCUs out of total 92 SNCUs in the states of
Rajasthan (n=59) and Odisha (n=33) were analyzed.
The SQCI for Odisha increased from 0.44 to 0.57 over a period of
one year while that of Rajasthan showed a marginal increase. (Table
II, Fig. 1). Overall, the mean difference of the
differences in the composite index of each unit between January
to March, 2016 and same period in 2017 was 0.20 (95% CI 0.13-
0.28; P<0.001). Similar results were obtained for other
indices. A significant improvement in the overall composite
score was noted in Odisha [MD (95% CI) 0.22, (0.11-0.33) P=0.003]
and Rajasthan [MD (95% CI) 0.17, (0.05-0.3) P=0.002]
(data not shown).
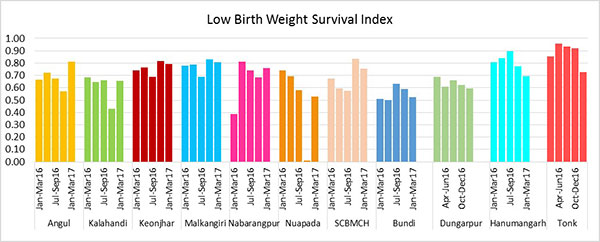
We analyzed the key indices that are most
amenable to improvement within the limited period of
intervention. Those indices were index for rational use of
antibiotics, index for mortality in normal weight babies and low
birth weight survival index. An analysis of every unit for the
difference in these indices for the same time periods showed a
significant improvement. A positive effect in terms of an
improvement in the overall composite score was observed one year
after the initiation of the QI model (data available at
https://sncuindiaonline.org).
Table II Indices to Measure Quality of Care in SNCUs in India Based on SQCI Model
| Time period |
SQCI |
Rational |
Index for |
Inborn birth |
Index for |
Low birth |
Low birth |
Optimal |
|
|
admission |
rational use |
asphyxia |
mortality in |
weight |
weight |
bed |
|
|
index |
of antibiotics |
index |
normal weight |
admission |
survival |
utilization |
|
|
|
|
|
babies |
index |
index |
index |
| Odisha (7 SNCUs combined) |
|
|
|
|
|
|
|
|
| I qtr 2016 |
0.44 |
0.91 |
0.34 |
0.70 |
0.40 |
0.27 |
0.66 |
0.20 |
| II qtr 2016 |
0.28 |
0.95 |
0.01 |
0.64 |
0.44 |
0.26 |
0.71 |
0.28 |
| III qtr 2016 |
0.46 |
0.95 |
0.41 |
0.62 |
0.17 |
0.33 |
0.65 |
0.47 |
| IV qtr 2016 |
0.44 |
0.94 |
0.42 |
0.62 |
0.09 |
0.34 |
0.66 |
0.63 |
| I qtr 2017 |
0.57 |
0.99 |
0.50 |
0.69 |
0.36 |
0.27 |
0.81 |
0.74 |
| Rajasthan (4 SNCUs combined) |
|
|
|
|
|
|
|
|
| I qtr 2016 |
0.50 |
0.74 |
0.55 |
0.79 |
0.71 |
0.19 |
0.67 |
0.27 |
| II qtr 2016 |
0.40 |
0.76 |
0.11 |
0.90 |
0.87 |
0.18 |
0.71 |
0.20 |
| III qtr 2016 |
0.40 |
0.73 |
0.12 |
0.89 |
0.69 |
0.19 |
0.76 |
0.20 |
| IV qtr 2016 |
0.49 |
0.78 |
0.29 |
0.89 |
0.71 |
0.21 |
0.70 |
0.35 |
| I qtr 2017 |
0.52 |
0.80 |
0.51 |
0.82 |
0.67 |
0.20 |
0.62 |
0.39 |
| MD (95% CI) a |
0.20 |
0.07 |
0.28 |
-0.01 |
-0.33 |
0.008 |
0.01 |
0.14 |
|
(0.13-0.28)b |
(0.03-0.11)b |
(0.16-0.41)c |
(-0.05-0.03) |
(-0.52,-0.14)b |
(-0.02--0.03) |
(-0.09-0.12)b |
(0.007- 0.27)b |
| aMean difference in
scores in each unit in first quarter of 2016 and 2017;
bP<0.05; #P<0,001, SNCU: Special newborn care unit;
SQCU: SNCU quality of care index; ^I quarter:
January-March, II quarter: April-June, III quarter:
July-September, IV quarter: October-December. |
DISCUSSION
This study describes the development of a
composite index and its application in two states of India. Our
results showed SQCI in the SNCUs could be utilized for improving
quality of services. An analysis of the SQCI over a period of
one year showed a significant improvement in both the states.
Our findings demonstrate that program
managers can use the tool to monitor the FBNC program. In the
state of Rajasthan, the SQCI scores were utilized to initiate
discussions on the challenges and discuss areas for improvement
such as rational use of antibiotics, admission criteria and
inpatient management of LBW newborns. Similarly, in Odisha, this
model was used to identify and prioritize the shortfalls that
were addressed during supportive supervision by the medical
officers as part of the routine program.
Globally, it is now known that quality
improvement (QI) models work in diverse cultures and locations
[15]. Studies have shown that a regular system of QI
intervention generally leads to improved adherence to health
care delivery practices [8,12,13]. A QI project in six tertiary
care hospitals in India, focused on interventions for increasing
awareness on health care associated infections, improving
compliance to infection control measures and monitoring rational
antibiotic use reported. Periodic visits, rapid assessments and
feedback, training and action at public health facilities has
been reported to lead to improvement in adherence to QI
guidelines in labor rooms in Rajasthan [8]. Periodic monitoring
of labor rooms and newborn care facilities in Bihar also
resulted in favorable outcomes [13,17]. Though on-site real time
observations to assess quality of delivery of services have
their own merits, yet it is a cost-and-resource intensive
exercise and hence, may not be a preferred option for public
health program [13].
Several QI models that have attempted to
improve the quality of services have focused on babies with LBW
[18-21]. The goals of these models were to identify and explain
variations in clinical practices and patient outcomes from the
routinely collected secondary data on newborns weighing less
than 1500g [19]. Our assessment is based on the online database
maintained by the health system, which is similar to those
models. In our country, the purpose of setting up SNCUs was to
take care of LBW babies primarily. However, reports suggest that
the bulk of admissions to SNCUs are contributed by babies whose
birthweights are more than 2500 [5,6]. Our approach therefore
included babies of all birth weights.
An advantage of our approach is the ease with
which data can be assembled and analyzed without relying on any
special technical help. In our case, concurrently and routinely
collected data from SNCUs were used which was independent of the
process of medical records data abstraction. The indicators used
to calculate SQCI are objective in nature, and less likely to be
influenced by individual perceptions. Another advantage of our
approach is that every SNCU in-charge in the country has access
to review their own performance through the online portal, which
is an advantage in terms of efficiency and feasibility.
Our limitations were that we captured only
the providers’ performance and users’ perspectives were
completely missed out. Although an important component in itself
[22], we did not include them due to feasibility issues. Certain
indices such as newborns discharged within 24 hour do not
capture the reasons for admission, which is a drawback.
Secondly, an independent evaluation to assess the validity of
SQCI indices was not undertaken and it remains a limitation. In
order to obtain some feedback on the reliability of SQCI,
trained neonatologists did an independent assessment of select
SNCUs, although this was not very objectively done. The overall
feedback given by the experts confidentially corroborated well
with the inferences drawn based on data driven QI model. Our
experiences from 11 SNCUs across two states represent diverse
locations lending to a possible generalizability with states
with similar health indicators.
Government at both national and state levels
were in support of QI initiatives using SQCI. Use of an existing
mechanism of surveillance without any major external support for
QI makes it more feasible as compared to the existing QI models.
Implemented within the existing health systems, infrastructure
and human resources, it contains a few components that can be
easily added onto the existing system.
The SQCI index is a useful tool to evaluate
the quality of neonatal care services in the Indian Special
Newborn Care Units. The index can be used to follow a unit’s
performance over time or to benchmark various units and for
quality improvement.
Contributors: HK: conceptualized SQCI and
provided technical oversight of the process of SQCI analysis and
use; RK: developed the statistical model during
conceptualization of SQCI, analyzed data, interpreted the
results and contributed to writing of the manuscript. VA,AK:
provided technical support during conceptualization of SQCI,
monitoring indicators and reviewed the manuscript; AAB:
contributed in the framing of monitoring indicators and reviewed
the manuscript SBN: reviewed the literature and drafted the
manuscript; PC,PKS: implemented SQCI in their respective states,
reviewed manuscript and provided inputs.
Funding: This study was conducted as part
of the Newborn care project supported by Norway India
Partnership Initiative (NIPI); Competing interest: None
stated.
|
|
WHAT IS ALREADY KNOWN?
•
There are multiple methods available to assess
quality of services from routinely collected data.
WHAT THIS STUDY ADDS?
•
It is possible to calculate indices (SQCI) based on
available data that serve as proxy to quality of
services.
•
It is feasible to implement SQCI in public health
settings for quality improvement.
|
REFERENCES
1. Facility based newborn care:
Operational guidelines. In: Ministry of Health and Family
Welfare, editor. New Delhi: Ministry of Health and Family
Welfare, Government of India; 2011.
2. Ministry of Health and Family Welfare.
Health Management Information System. In: Ministry of
Health and Family Welfare, editor. Ministry of Health and Family
Welfare, Govt of India; 2017.
3. MOHFW. Special Newborn Care Units in
India. In: Ministry of Health and Family Welfare, editor.
New Delhi 2017.
4. Strengthening Facility Based Paediatric
Care: Operational Guidelines for Planning & Implementation in
District Hospitals. In: Child Health Division, Ministry
of Health and Family Welfare, Government of India, New Delhi.
September 2015. Accessed on November 16, 2020. Available from:
https://nhm.gov.in/images/pdf/
programmes/child-health/guidelines/Strenghtening_FacilityBasedPaediatric
Care-OperationalGuidelines.pdf
5. Neogi SB, Malhotra S, Zodpey S, Mohan P.
Assessment of special care newborn units in India. Health Pop
Nutr. 2011;29:500-9.
6. Neogi SB, Malhotra S, Zodpey S, Mohan P.
Challenges in scaling up of special care newborn units-Lessons
from India. Indian Pediatr. 2011;48:931-5.
7. Sharma G, Powell-Jackson T, Haldar K,
Bradley J, Filippi V. Quality of routine essential care during
childbirth: Clinical observations of uncomplicated births in
Uttar Pradesh, India. Bull World Health Organ. 2017;95:419-29.
8. Iyengar K, Jain M, Thomas S, et al.
Adherence to evidence based care practices for childbirth before
and after a quality improvement intervention in health
facilities of Rajasthan, India. BMC Pregn Childbirth.
2014;14:270.
9. Chauhan M, Sharma J, Negandhi P, Reddy S,
Sethy G, Neogi S. Assessment of newborn care corners in selected
public health facilities in Bihar. Indian J Public Health.
2016;60:341-6.
10. Chawla D, Suresh GK. Quality improvement
in neonatal care - A new paradigm for developing countries.
Indian J Pediatr. 2014;81:1367-72.
11. Neogi SB, Malhotra S, Zodpey S, Mohan P.
Does facility-based newborn care improve neonatal outcomes? A
review of evidence. Indian Pediatrics. 2012;49:651-58.
12. Sarin E, Kole SK, Patel R, et al.
Evaluation of a quality improvement intervention for obstetric
and neonatal care in selected public health facilities across
six states of India. BMC Pregn Childbirth. 2017;17:134.
13. Neogi SB, Shetty G, Ray S, Sadhukhan P,
Reddy SS. Setting up a quality assurance model for newborn care
to strengthen health system in Bihar, India. Indian Pediatr.
2014;51:136-8.
14. Vagias WM. Likert -type scale response
anchors. Clemson University: Department of Parks, Recreation and
Tourism Management, 2006.
15. Nadeem E, Olin SS, Hill LC, Hoagwood KE,
Horwitz SM. Understanding the components of quality improvement
collaboratives: a systematic literature review. Milbank Q.
2013;91:354-94.
16. Mehndiratta A. Quality Improvement of
Facility Based New Born Care in India: ACCESS health
International; 2014; Available from: http://accessh.org/wp-content/uploads/2014/07/Quality-Improvement-of-Facility-Based-Newborn-Care-in-India-Poster.pdf
17. Sharma J, Neogi S, Negandhi P, Chauhan M,
Reddy S, Sethy G. Rollout of quality assurance interventions in
labor room in two districts of Bihar, India. Indian J Public
Hlth. 2016;60:323-8.
18. Horbar JD. The Vermont Oxford Network:
Evidence-based quality improvement for neonatology. Pediatrics.
1999;103:350-9.
19. Horbar JD, Rogowski J, Plsek PE, et al.
Collaborative quality improvement for neonatal intensive care.
NIC/Q Project Investigators of the Vermont Oxford Network.
Pediatrics. 2001;107:14-22.
20. Hernández-Borges AA, Pérez-Estévez E,
Jiménez-Sosa A, et al. Set of quality indicators of pediatric
intensive care in Spain: Delphi method selection. Pediatr Qual
Safety. 2017;2:e009.
21. Profit J, Zupancic JA, Gould JB, et al.
Correlation of neonatal intensive care unit performance across
multiple measures of quality of care. JAMA Pediatr.
2013;167:47-54.
22. Lachman P, Jayadev A, Rahi M. The case
for quality improvement in the neonatal intensive care unit.
Early Human Dev. 2014;90:719-23.
|
|
|
 |
|