|
|
|
Indian Pediatr 2015;52: 357 |
 |
Congenital Platelike Osteoma Cutis
|
|
#Sidharth Sonthalia and
*Archana Singal
Departments of Dermatology, #Kalyani-Escorts Hospital,
Gurgaon; and *UCMS & GTB Hospital, Delhi; India.
Email: #
[email protected]
|
|
An 11-month-old infant was evaluated for gradually enlarging localized
swellings over the left side of the chest, present since birth. The
perinatal, developmental and family history were unremarkable. Cutaneous
examination revealed two well-defined porcelain white-colored,
plate-like hard, subcutaneous swellings over the left upper lateral
chest wall, measuring 15×20 mm and 5×10 mm (Fig. 1). The
swellings were non-tender, free from underlying structures and without
any visible discharge. There was no clinical evidence of rickets. Serum
and urinary levels of calcium and phosphorus, and serum parathyroid
hormone levels were normal. A chest radiograph revealed two prominent
spicules of calcification in the soft tissue of left lateral chest wall
at the level of 10th rib. A diagnosis of congenital plate-like osteoma
cutis was confirmed on excisional biopsy that revealed dermal
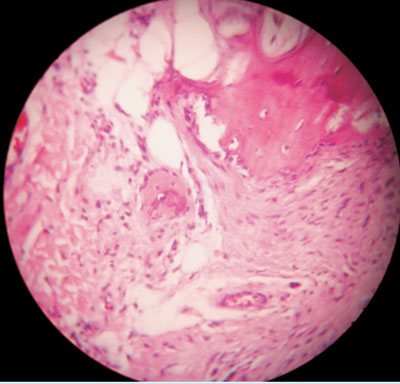
ossification with multiple osteocytes (Fig. 2).
 |
 |
|
Fig. 1 Porcelain white-colored,
plate-like, subcutaneous swellings over the left upper lateral
chest wall.
|
Fig. 2 Dermal ossification with
multiple osteocytes in oval-shaped lacunae (hematoxylin & Eosin,
400×).
|
Four types of osteoma cutis have been identified –
congenital plaque- or plate-like, late-onset osteoma, widespread
osteomas, and multiple miliary facial osteomas. Plaque-like osteoma is
present since birth. Although the scalp and extremities are commonly
affected, any site may be involved. In osteoma cutis, bone arises in
skin and soft tissues through membranous ossification, purportedly
effected by osteoblastic differentiation of dermal fibroblasts. Clinical
diagnosis is confirmed on plain radiography and histopathology of the
excised specimen. Serum calcium and parathyroid hormone levels aid in
ruling out Albright’s hereditary osteodystrophy. Surgical excision is
the mainstay of treatment.
|
|
|
 |
|
