|
|
|
Indian Pediatr 2013;50: 423-424 |
 |
Angioedema Following Ingestion of Fried Flying
Red Fire Ants
|
|
V Nandhakumar
From Department of Pediatrics, Melmaruvathur
Adhiparasakthi Institute of Medical Sciences Hospital, Melmaruvathur,
Kancheepuram, Tamilnadu 603 319, India.
Correspondence to: Dr V Nandhakumar, B-6,
Lakshmi apartments, Meenambal Street, Melmaruvathur,
Kancheepuram, TN 603 319, India.
Email:
[email protected]
Received: September 18, 2012;
Initial review: September 24, 2012;
Accepted: October 31, 2012.
|
|
Red ants’ sting anaphylaxis was rarely
reported from India. But angioedema due to ingestion of fried "flying
red fire ants" in children is almost never reported from India and also
very rarely reported from outside India. We report a case of recurrent
non allergic angioedema following ingestion of fried flying red ants.
Key words: Angioedema, Fried flying red ants,
Ingestion, Child.
|
Red fire ant (Solenopsis Geminata
Fabricius) sting can cause allergy from local reactions
to anaphylaxis [1]. However, angioedema due to
ingestion of cooked ‘flying red fire ants’ in children has
not been reported earlier.
Case Report
An 8-year-old boy was rushed to the
pediatric emergency room of our hospital with the complaints
of rapidly progressive swelling of within last 5 minutes.
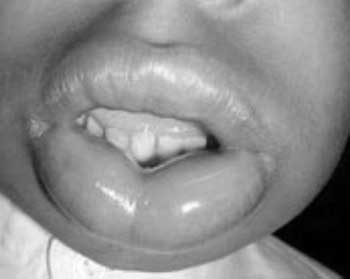
Swelling of face was first noticed in lips (Fig.1),
periorbital region, ear lobules and then rapidly progressed
to entire face. There was no history of breathlessness, pain
or itching. There was no rash, but angioedema of face was
noted. His vital parameters were normal. Mother gave the
history of ingestion of fried flying ants (Fig. 2).
 |
|
Fig. 1 Angioedema of lips.
|
 |
|
Fig.2 Fried flying red fire
ants.
|
The reasons behind the ingestion of
flying ants given by the mother were high iron content,
improve the fertility status of the person and good taste.
She also gave the past history of similar event but of
lesser severity, since last one year. No other family
members developed allergy or angioedema on ingesting the
same dish. Investigations showed normal total count of
8300/mm 3,
differential count of P58, L34, M1 and E7 and absolute
eosinophil count of 250/mm3.
Serum C1 esterase level was normal. Urine examination and
renal function tests at admission and discharge were within
normal limits.
The child was treated with intravenous
hydrocortisone and antihistaminics. Edema started to
decrease after 4 hours of management and the child recovered
fully by 24 hours.
Discussion
Insects of the order hymenoptera, members
of genus Solenopsis namely S. invicta, S richteri
and S geminate, have a stinging apparatus at the tail
end of their abdominal segment and are capable of delivering
100 ng of venom. The venom has various peptide and protein
components and some of which are capable of inducing
vasoreactive substances. It has been estimated that 1500
stings would be required to deliver a lethal dose of
hymenoptera venom for a non allergic adult weighs 70 kg [2].
Ninety-nine percent of the alkaloid component of red
fire-ant venom is made up of 2, 6, di-substituted
piperidines that have hemolytic, antibacterial,
insecticidal, and cytotoxic properties. Venom alkaloids do
not generate IgE antibody responses and thus do not appear
to be responsible for allergic reactions [3]. Anaphylaxis is
more common and severe in subsequent stings [4]. Serious
complications like laryngospasm, seizures, rhabdomyolysis
and acute renal failure were reported [5].
Allergic angioedema typically occurs
within several minutes of exposure to insect stings. In the
above case angioedema started after 5 hours of exposure
without pruritus and urticarial rash suggesting non allergic
etiology due to excess bradykinin release. The close
differential diagnosis is C1 esterase inhibitor deficiency,
either hereditary or acquired, causing angioedema. This was
ruled out in the above case by normal C1 esterase inhibitor
level. The etiology of red ants’ ingestion was concluded
also on the basis of recurrent presentation on exposure to
the same.
References
1. Havaldar PV, Patil SS, Phadnis C.
Anaphylaxis due to red fire ant bite. Indian Pediatr. 2012;
49:237-8.
2. Freeman TM. Hypersensitivity to
hymenoptera stings. N Engl J Med. 2004;351;1978-84.
3. DeShaze RD, Butcher BT, Banks WA.
Reactions to the stings of imported fire ant. N Engl J Med.
1990;323:462-6.
4. Goddard J, Jarratt J, de Castro FR.
Evolution of the fire ant lesion. JAMA. 2000;284:2162-3.
5. Koya S, Crenshaw D, Agarwal A. Rhabdomyolysis and
acute renal failure after fire ant bites. J Gen Intern Med.
2007;22:145-7.
|
|
|
 |
|
