|
|
|
Indian Pediatr 2011;48:
289-293 |
 |
Effect of Iron and Zinc Deficiency on Short
Term Memory in Children |
|
K Umamaheswari, Mythily Bhaskaran, Gautham Krishnamurthy, Hemamalini*and
Kavita Vasudevan
†
From Department of Physiology, Madras Medical College,
Chennai; *Billroth Hospital, Chennai, Tamil Nadu; and
†Department of Community Medicine, AV Medical College, Puducherry; India.
Correspondence to: Dr K Umamaheswari, No 33, East Main
Road, Venkateshwara Nagar, Puducherry 605 013, India. Email:
[email protected]
Received: July 1, 2009;
Initial review: August 18, 2009;
Accepted: March 29, 2010.
Published online 2010 August 1.
PII: S097475590900459-1
|
Objective: To evaluate the effect of iron and zinc deficiency on short
term memory of children in the age group of 6-11 years and to assess the
response to supplementation therapy.
Design: Interventional study.
Setting: 100 children in the age group of 6-11
years (subdivided into 6-8 yr and 9-11 yr groups) from an urban
corporation school.
Methods: After collection of demographic data, the
study children underwent hematological assessment which included serum
iron, serum zinc, and hemoglobin estimation. Based on the results, they
were divided into Iron deficient, Zinc deficient, and Combined deficiency
groups. Verbal and nonverbal memory assessment was done in all the
children.
Intervention: Iron (2mg/kg bodyweight in two
divided doses) and zinc (5mg once-a-day) supplementation for a period of 3
months for children in the deficient group.
Results: All children with iron and zinc deficiency
in both the age groups had memory deficits. Combined deficiency in 9-11
years group showed severe degree of affectation in verbal (P<0.01)
and non-verbal memory (P<0.01), and improved after supplementation
(P = 0.05 and P<0.01, respectively). In 6-8 years group,
only non-verbal form of memory (P =0.02) was affected, which
improved after supplementation.
Conclusion: Iron and zinc deficiency is associated
with memory deficits in children. There is a marked improvement in memory
after supplementation. Post supplementation IQ scores do not show
significant improvement in deficient groups in 6-8 year olds.
Key words: Child, India, Iron, Non-verbal memory,
Supplementation, Verbal memory, Zinc.
|
|
M
icronutrient deficiencies are
widespread in many developing countries and are common among young persons
hailing from low socioeconomic groups [1-3]. Children are particularly at
risk for such deficiencies as a result of excessive losses of iron and
zinc due to parasitic infections [4,5]. Such deficiencies can have
far-reaching health consequences, contributing to impairments in growth,
neurobehavioral function, and immune competence, and increases in
morbidity and mortality [6,7]. Of the micronutrients, the two
micronutrients that have been found to be highly prevalent and linked to
cognitive functioning are iron and zinc. Studies have shown that
iron-deficient children lag behind controls in terms of anthropometric
parameters, cognitive status and various athletic events performed [8-10].
In the case of iron deficiency, whether associated with anemia or not, the
results of treatment trials have been conflicting in nature and have been
linked to small sample size or lack of placebo group [7], and most of them
have concentrated on iron deficient anemia rather than iron deficiency
per se. Zinc has been causally linked to various diseases such as
diarrhea and pneumonia, but there have been few studies that have studied
the impact of zinc deficiency on cognition [11,12]. This study was
undertaken with the objective of identifying the role of iron, zinc, and
combined iron and zinc deficiency on verbal and nonverbal subsets of
memory, and to determine the difference in the affectation of memory
between 6-8 and 9-11years age group.
Methods
This study was conducted during the period from
December 2005 to August 2006 at the Government primary school, Porur,
Chennai, having students primarily belonging to the upper low
socioeconomic background, as assessed by revised Kuppuswamy scale [13].
Permission was obtained from the Dean, Madras Medical College; the
Assistant Elementary Education Officer; and Principal, Government Primary
School, Porur. This study was approved by the college Ethical Committee.
Written informed consent was taken from the parents of children who
participated in the study.
One hundred randomly selected children of both sexes in
the age group of 6 to 11 years were enrolled for the study and subjected
to hematological tests and memory assessment. Children with infection,
fever, history of drug intake for any illness, and girls who had attained
menarche, were excluded. They were grouped into 6-8 years (Group A; n=40)
and 9-11 years (Group B; n=60). Further sub grouping was done based
on hematological results. The tests included hemoglobin estimation
by Cyanmethemoglobin method, serum iron and total iron binding capacity (TIBC)
by colorimetric method, serum ferritin by Elisa, and serum zinc by atomic
absorption spectrophotometry [14,15]. Intelligence was assessed using the
Binet-Kamath scale.
Based on serum iron levels, total iron binding capacity
(TIBC), serum ferritin and serum zinc values, the children were
categorized as Iron deficient (serum iron <60 meq/dL, TIBC
³360,
serum ferritin £10
mg/dL and serum zinc >65 mcg/dL) and Zinc deficient (serum iron
³60
mcg/dL, TIBC <360, serum ferritin
£10
mg/dL and serum zinc £65
mcg/dL). Those with values suggestive of both iron and zinc deficiency,
were categorized as Combined deficient, and all others were considered
Normal.
 |
|
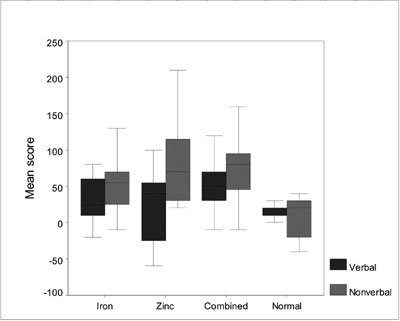
Fig. 1 Box and whisker plot showing
significant memory improvement of 9-11yrs children in the combined
deficiency Group and zinc deficiency Group. |
Tests for Memory
Six tests were selected, which were generated from
different sources [16], including Wechsler memory scale, Mini mental state
examination, Mann-Buitar visual memory screen, and Catel’s
retentivity test, as described below.
Digit forward: The subject is instructed to
recite digit sequences of increasing length in the order presented.
Sentence repetition: Five sentences are
presented one by one to the subject for immediate reproduction.
Story recall: The logical memory test is
used to examine the subject’s immediate verbal memory. The examiner reads
the story to the child and the child is asked for immediate recall after
hearing the story.
Picture recall: Here a row of picture is shown. The
examiner then covers the pictures. Then the subject is asked to list the
pictures exactly in the same order they saw starting at one end of row
each time.
Benton visual retention test: It is a recall
of 10 complex and unfamiliar geometrical figures. It has 10 designs
on 10 cards. Each design is explored for 10 seconds and the subject
is asked to reproduce the design immediately from memory.
Cattell’s retentivity test: A card is shown
on which 10 geometrical figures are drawn. The subject is allowed to look
at them for 30sec and after 2minutes a second card is shown from which the
figures that were shown should be identified.
Children who were deficient in iron and zinc were given
the following supplements depending on the nutrient(s) they were deficient
in: Ferrous sulphate tablets - 2 mg/kg body weight [17], Zinc - 5 mg
equivalent once-a-day in the form of syrup: and children deficient in both
the minerals were given both tablet and syrup for a period of 3 months.
The normal children were advised nutritious food during the study period.
The tests were repeated after supplementation for three
months. Due to drop outs, only 81 students continued in the study. Before
supplementation, hematological results indicated an evident correlation
between serum iron, total iron-binding capacity and serum ferritin levels.
Taking this into consideration and the financial constraints, serum iron
was alone performed for estimating iron deficiency. Serum zinc was also
estimated.
Results
Sixty-seven of the 100 students in the study were found
to be deficient in iron and 43 were deficient in zinc. 35% of 6-8 years
and 32% in 9-11 years of age were iron deficient, 10% of 6-8 years and
8.3% in 9-11 years of age were zinc deficient. The incidence of combined
deficiency of both iron and zinc were found to be 35% in 6-8 years and
33.3% in 9-11years.
TABLE I
Memory Scores in Different Groups Before Supplementation
| |
Iron |
Zinc |
Combined |
Normal |
P |
| |
Deficiency |
Deficiency |
Deficiency |
|
value |
|
6-8 years |
|
Verbal memory |
161 ± 74.6 |
175 ± 35.3 |
130 ± 41.2 |
250 ± 10.0 |
0.07 |
|
Non-verbal memory |
146 ± 64.4 |
115 ± 21.2 |
120.9 ± 83.4 |
245 ± 7.0 |
0.02 |
| IQ |
100 ± 5.5 |
95 ± 4.2 |
96.6 ± 4.7 |
107.5 ± 0.7 |
0.03 |
|
9-11 years |
|
Verbal memory |
171.5 ± 66.3 |
205.7 ± 49.2 |
156 ± 57.2 |
227.1 ± 39.6 |
<0.01 |
|
Non-verbal memory |
132 ± 57.5 |
120 ± 27.6 |
117.3 ± 24.3 |
234.2 ± 41.2 |
<0.01 |
| IQ |
98.9 ± 5.5 |
94.8 ± 4.05 |
94.7 ± 2.3 |
107.2 ± 4.2 |
<0.01 |
|
Significance by
Mann-Whitney U test; All values are mean ± SD. |
Non verbal memory and IQ assessment showed affectation
mainly in the iron deficient and combined deficient groups in the 6-8
years age group. Significant affectation of verbal, nonverbal memory and
IQ was seen in 9-11 years age group and the greater mean score difference
in the combined deficient group (Table I). Improvement was
seen in the verbal, non verbal memory and IQ mainly in the 9-11 years age
group, more so in the combined deficient groups as indicated by the
difference in the mean scores obtained (Table II).
TABLE II
Improvement in Memory Scores After Supplementation
| |
Iron |
Zinc |
Combined |
Normal |
P |
| |
deficiency |
deficiency |
deficiency |
|
value |
|
6-8 years |
|
Verbal memory |
38 ± 35.5 |
40 ± 28.2 |
70.9 ± 41.8 |
20(12.7) |
<0.01 |
|
Non-verbal memory |
33 ± 22.3 |
50 ± 46.5 |
56.3 ± 37.7 |
30(14.14) |
0.49 |
| IQ |
8.0 ± 2.3 |
6 ± 1.3 |
3.8 ± 5.3 |
8.5(6.3) |
0.27 |
|
9-11 years |
|
Verbal memory |
30.5 ± 29.2 |
20 ± 5.9 |
50.6 ± 37.5 |
14.2 ± 2.3 |
0.05 |
|
Non-verbal memory |
55.5 ± 39.1 |
84.2 ± 69.7 |
72 ± 44.7 |
11.4 ± 6.4 |
<0.01 |
| IQ |
3.97 ± 2.1 |
12.4 ± 3.3 |
5.01 ± 3.9 |
2.5 ± 1.5 |
0.05 |
Significance by Mann-Whitney U test; All values represent mean ±(SD).
|
Discussion
Nutritional anemia is a syndrome and not a disease
entity caused by malnutrition in its widest sense. It has been defined by
WHO as a condition in which the hemoglobin content of blood is lower than
normal as a result of deficiency of one or more essential nutrients [18].
It was also found that estimation of hemoglobin alone could not detect
mild forms of iron deficiency which were found out by implementing the
criteria involving all tests estimating iron-related indices (serum iron,
serum ferritin, iron binding capacity and transferrin saturation). Thus it
is vital to differentiate between iron deficiency alone and that
associated with anemia, and there have been earlier studies taking this
factor into consideration. On supplementation for a period of three
months, it was found that all the children in deficient population reached
the normal blood values.
Tests of verbal memory assess the immediate verbal
memory which does not require any analytical component but only simple
immediate repetition. Studies have shown lower values in Wechsler
intelligence scale for children of 6-8 years for items on verbal and
performance subtests which improved with iron supplementation [7].
Analysis of our scores shows that the verbal memory was affected in both
age groups, especially 9-11 years, with more severe affectation in the
combined deficiency group. After supplementation for 3 months, 6-8 years
age group showed marked improvement, particularly in the combined
deficiency group, suggesting a greater tendency to revert to the normal
growth.
Picture recall, Benton visual retention test and
Cattell retentivity test evaluate immediate memory and visuospatial
abilities using visual designs. They also require mental manipulation of
figures with physical effort and test the visual nonverbal memory. Otero,
et al. [19] observed significant impairment of visual memory in
anemic children when compared to non-anemic children, whereas with zinc
deficiency, there was no change in test scores when 5 year old children
were assessed for visual sequential memory [20]. Penland, et al.
[21] used extensive neuropsychologic battery of tests to asses cognitive
and psychomotor functions in 6-9 year old children and observed zinc
supplementation improved performance on tasks assessing visual recognition
memory. From our results in non verbal tests, it is evident that both age
groups are significantly affected in visual memory with more affectation
in the combined deficiency subgroup. The results indicate the dependence
of non verbal memory on both iron and zinc in both the age groups, in
contrast to verbal memory, which showed marked degree of affectation only
in the 9-11 years.
Post-supplementation all the groups in the 6-8 years
age group showed similar results, the zinc group and combined group of the
9-11 years age group showed better results than the normal indicating a
greater tendency of the zinc deficient to revert to normal.
Children of both the age groups showed IQ affectation
before supplement while significant improvement was noticed only in the
9-11 year age group, particularly in the combined deficiency group, after
supplementation.
The age for cultivating inspiration and wisdom is from
6-8 years, and 9-11 years is considered to be important in the formative
process and reasoning. This is the reason for the focus of our study in
this particular age group. Memory is an important tool for a good academic
performance and plays an important role in modifying the child’s potential
for learning, which influences behavior. We conclude that identification
of the deficiency at an early age and proper supplementation would prevent
severe memory loss in the later age. Deficiency in zinc is not uncommon
and has to be looked for on a routine basis as this mineral seems to
affect memory more than that caused by iron deficiency alone.
Acknowledgment: We thank the staff of Departments
of Biochemistry, and Physiology, MMC and Mr G Venkatesan, Lecturer in
Statistics, Clinical Epidemiology Unit, MMC for his statistical
assistance.
Contributors: MB: Conceived and designed the study
and revised the manuscript for important intellectual context. UK and GK
collected data and drafted paper, conducted laboratory tests and
interpreted them. UK also revised the manuscript for important
intellectual context. H: Analyzed the data and helped in manuscript
writing. Final manuscript was approved by all the authors.
Funding: None.
Competing interests: None stated.
|
What is Already Known?
• Iron deficiency is known to affect cognition in
6-11 year olds but the role of zinc deficiency in memory is
questionable.
What This Study Adds?
• Supplementation of iron and zinc was found to improve both
verbal and non-verbal memory.
|
References
1. Lozoff B. Iron deficiency and child development.
Food Nutr Bull. 2007;28:S560-71.
2. Tupe R, Chiplonkar SA, Kapadia-Kundu N. Influence of
dietary and sociodemographic factors on the iron status of married
adolescent girls from Indian urban slums. Int J Food Sci Nutr. 2008;7:1-9.
3. Misra S, Kantharia SL, Damor JR. Prevalence of
goitre in 6 -12 years school-going children of Panchmahal district in
Gujarat, India. Indian J Med Res. 2007;126:475-9.
4. Filteau SM, Tomkins AM. Micronutrients and tropical
infections. Trans R Soc Trop Med Hyg. 1994;88:1-3.
5. Koski KG, Scott ME. Gastrointestinal nematodes,
nutrition and immunity: Breaking the negative spiral. Annu Rev Nutr.
2001;21:297-321.
6. Viteri FE, Gonzalez H. Adverse outcomes of poor
micronutrient status in childhood and adolescence. Nutr Rev.
2002;60:S77-3.
7. Grantham-McGregor SM, Ani CC. The role of
micronutrients in psychomotor and cognitive development. Br Med Bull.
1999;55:511-27.
8. Shankar N, Tandon OP, Bandhu R, Madan N, Gomber S.
Brainstem auditory evoked potential responses in iron deficient anemic
children. Indian J Physiol Pharmacol. 2000;44:297-303.
9. Bhatia D, Seshadri S. Growth performance in anemia
and following iron supplementation. Indian Pediatr. 2003;40: 985-90.
10. Gowri AR, Sargunam HJ. Assessment of mental and
motor abilities of school going children with anemia. Indian J Nutr Dietet.
2005;42:99-105.
11. Black MM. Micronutrient deficiencies and cognitive
functioning. J Nutr. 2003;133:3927S-31.
12. Bhatnagar S, Taneja S. Zinc and cognitive
development. Br J Nutr. 2001;85 (Suppl 2):S139-45.
13. Kumar N, Shekhar C, Kumar P, Kundu A. Kuppuswamy’s
socioeconomic status scale-updating for 2007. Indian J Pediatr.
2007;74:1131-2 .
14. Virgil F, Fairbanks G, Klee G. Biochemical aspects
of haematology. In: Burtis CA, Ashwood ER, (editors). Tietz
Textbook of Clinical Chemistry, 3rd ed. Philadelphia, Pennsylvania: W.B.
Saunders Company. 1999. p.1698-1704.
15. Fielding J, CookJD, Hallbe L, Izak G.
International Committee for standardization in haematology: The
measurement of total and unsaturated iron binding capacity in serum. Br J
Haematol. 1978;38:281-94.
16. Malavika, Kumar V, Rajagopalan S. Micronutrient
fortification of salt and its effect on cognition in Chennai school
children. Asia Pac J Clin Nutr. 2007;16:505-11.
17. Soemantri AG, Pollitt E, Kim I. Iron deficiency
anemia and educational achievement. Am J Clin Nutr. 1985;42:1221-8.
18. Lokeshwar MR, Choudary VP. Anemia in children.
In: Parthasarathy A, Menon PSN, Nair MK, editors. IAP Text book of
Pediatrics, 3rd Ed. New Delhi: Jaypee Brothers Medical Publishers. 2007.
p.602-3.
19. Otero GA, Aguirre DM, Porcayo R, Fernandez T.
Psychological and electroencephalographic study in school children with
iron deficiency. Int J Neurosci. 1999; 99:113-21.
20. Tamura T, Goldenberg RL, Ramey SL, Nelson KG,
Chapman VR. Effect of zinc supplementation of pregnant women on the mental
and psychomotor development of their children at 5 y of age. Am J Clin
Nutr. 2003;77:1512-6.
21. Penland JG, Sandstead HH, Alcock NW, Dayal HH, Chen
XC, Li JS, et al. A preliminary report: effects of zinc and
micronutrient repletion on growth and neuropsychological function of urban
Chinese children. J Am Coll Nutr. 1997; 16:268-72.
|
|
|
 |
|
