|
|
Short Communications Indian Pediatrics 2008; 45: 315-318 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Descriptive Epidemiology of Dengue Transmission in Uttar Pradesh |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
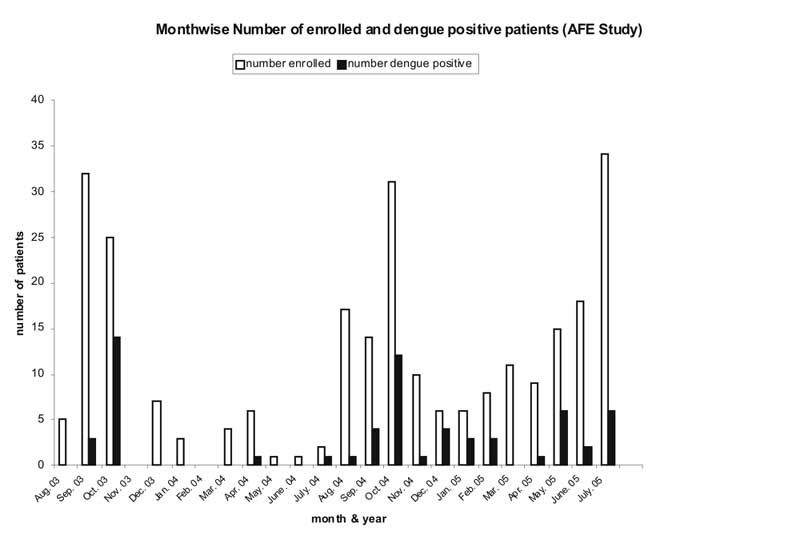
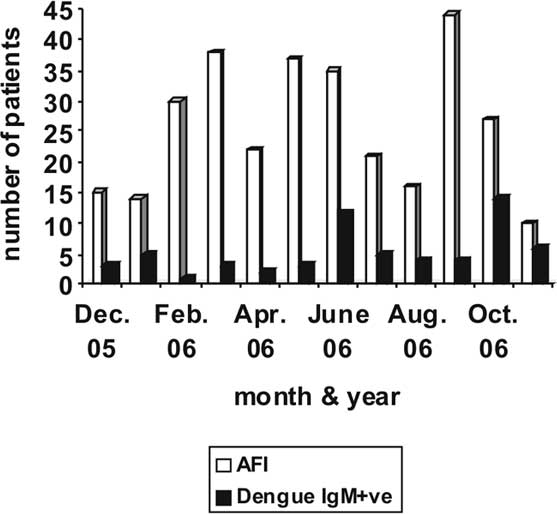
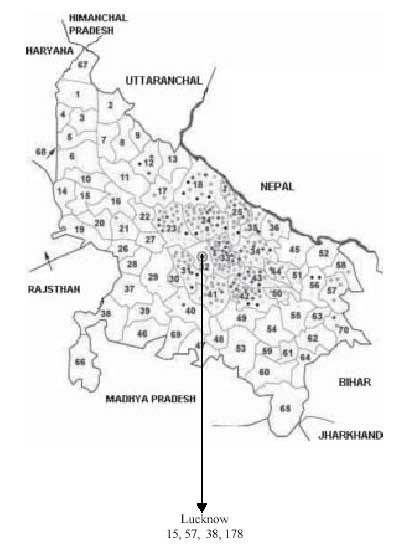
Introduction During the last decade, more frequent and severe epidemics of dengue have hit several Indian cities. Over the last few years we were engaged in a hospital based surveillance for dengue as part of 2 studies conducted here. A large number of patients were systematically screened for dengue infection. Since both the studies throw light on the epidemiology of dengue, this aspect of both studies is combined here to report the descriptive epidemiology of dengue infection in and around Lucknow. Methods The work was based at the Department of Pediatrics, King George Medical University, Lucknow. Over a period of 3 years from 2003 to 2006 we actively looked for indicators of dengue infection in patients presenting with (i) acute febrile encephalopathy (AFE) (2003-2005) and (ii) acute undifferentiated febrile illness (AUFI) (2005-2006) . AFE study: AFE was defined as fever with altered consciousness of 2 weeks duration or less in a previously well child. In July 2003, we launched a study to define the role of dengue encephalopathy in children presenting with AFE. Consecutive children between 1-12 years of age hospitalized with AFE were screened for dengue infection. Those children with a firm diagnosis of bacterial or tubercular meningitis(1,2) and hepatic encephalopathy were excluded. AUFI study: In 2005-2006, another study was conducted to examine the importance of dengue fever (DF) as a cause of AUFI among children presenting as outpatients. Consecutive children aged 6 months to 12 years reporting as outpatients on 3 preselected week days and seeking care for the complaint of fever of 15 days or less duration were enrolled in the study if they had no localizing signs of infection. In both studies, serum was tested for dengue IgM antibodies by antibody capture ELISA using commercial kits (Panbio, Australia) and in some cases in 2003 haemagglutination inhibition (HI) test in paired sera was performed by standard methods(3). Detailed addresses of the patients were noted down. The residence of the child could be divided into (i) rural or (ii) urban/periurban (amalgamation) areas. Age-sex, rural-urban, districtwise and month-wise distribution of cases was computed. Ethical Approval for both studies was obtained from India-CLEN IRB and KG Medical University Ethics Committee. Verbal consent was obtained from parents. Results A total of 265 of 612 patients presenting with AFE were enrolled. Forty nine patients underwent HI test in paired sera and 238 were tested for dengue IgM ELISA. A total of 62 patients were positive for dengue antibodies by either or both tests. For the AUFI study a total of 298 of 915 patients with fever were enrolled, of which 56 were positive for dengue IgM by ELISA. Thus a total of 118/563 (20.9%) patients seen over 3 years were positive for dengue antibodies. Table I and II show the age-sex and rural-urban distribution of enrolled and dengue positive cases. Figure 1 and 2 shows the monthwise enrollment and Figure 3 shows the districtwise distribution of enrolled and dengue positive cases. TABLE I Age and Sex Distribution of Enrolled and Dengue Antibody Positive Children
* Male: Female proportion in enrolled vs. antibody positive children was comparable for all age groups (P>0.05). Figures in parentheses indicate percentage. TABLE II Rural Urban Distribution of Enrolled and Dengue Antibody Positive Children
* Comparison of proportions (rural) between all enrolled and dengue antibody positive subgroup by Chi-square test.
Discussion This hospital based study shows presence of antibodies to dengue in a high proportion of AFE and AUFI patients, indicating active dengue transmission in the study area. Chances of cross-reactions with other flaviviruses are small(4). In the absence of community-based studies, this data may serve as an useful measure of epidemiology of the infection. We did not ask for travel history in our patients and expect that any differences in transmission area caused by recent travel would be minor. Dengue has traditionally been held to be a disease of high population density tropical urban areas(5,6). The proportion of rural and urban patients among those testing antibody-positive more or less paralleled the rural-urban ratio of enrolled patients indicating that dengue transmission is occurring equally in rural and urban areas. Over the last 1-2 decades there are increasing reports of dengue cases and outbreaks from rural areas in southern and western India(7-15). A single study from north India describes an outbreak of DF in rural Haryana(16). These outbreaks were investigated in a small number of patients with dengue antibody estimations. Ours is the first report in which such a large number of subjects were studied systematically over a period of three calendar years and the first report of dengue from rural Uttar Pradesh. The district-wise distribution showed that dengue occurred uniformly in the catchment area without areas of predilection. Many factors can be responsible for transmission in rural areas. Uttar Pradesh has a huge population, mostly living in rural areas. Unlike rural areas of other parts of the world, population density here is high. The residential parts of villages are water logged in the rainy season and breeding of the insect vector in water filled containers in and around the rural dwellings is likely. Contributors: RK conceived the study, wrote the research proposals, supervised data collection and paper writing. PT conducted ELISA tests and wrote the paper. ST conducted HI and ELISA tests. JJT collected clinical data. VV supervised antibody estimations. All authors helped in writing and approving the final draft. Funding: USAID/INCLEN. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()