|
|
Short Communications Indian Pediatrics 2008; 45:-312-314 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
A Simple Circuit to Deliver Bubbling CPAP |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
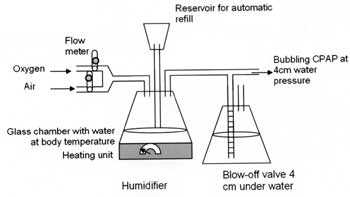
Introduction In the quest to bring down the neonatal mortality rate, the challenge is to develop low cost technology that can be used in remote settings(1,2). It is known that early use of continuous positive airway pressure (CPAP) reduces the incidence of chronic lung disease(3) and it may be used as an alternative to intubation and ventilation is some cases(4-7). Recent literature suggests that ‘bubbling CPAP’ is better than conventional CPAP. The bubbling CPAP is a form of oscillatory pressure delivery in which mechanical vibrations are transmitted to the chest secondary to non-uniform flow of gas bubbles across the downstream of a water seal(8) and this system results in waveforms similar to those produced by high-frequency ventilation when recorded by a transducer attached to the infant’s airway. The chest vibrations produced contribute to gas exchange by facilitated diffusion(9). We describe a circuit which delivers bubbling CPAP, is easy to assemble and can be adapted for use in any health facility where oxygen and compressed air are available. Methods In its most basic form, pressurized oxygen from an oxygen cylinder is delivered to the nasopharynx of the baby. An under water ‘T tube’ that acts as a blow off valve is interposed between the oxygen source and the baby. Adjusting the height of the water column above the exit of the ‘T tube’ can regulate the pressure in the system and the amount of CPAP delivered to the baby. The constant bubbling of gas through the blow off mechanism delivers the bubbling CPAP effect. Oxygen may be delivered by nasal prongs or more cheaply by a shortened endotrachel tube or a nasopharyngeal catheter (8F) inserted into the nose to a depth equal to the distance from the side of the nose to the front of the ear so the tip of the catheter is just visible in the pharynx below the soft palate when the mouth of the infant is open(10). This system however delivers 100% oxygen and can harm premature babies. The system can be modified by having a Y tube deliver a mixture of air and oxygen from 2 separate cylinders. Flow meters indicate the flow rate of the gases and the relative concentration of oxygen. A humidifier can also be added so the gas mixture is not dry and it does not irritate the airway. This humidifier consists of a heating element that keeps the water at 37degrees centigrade and the air that passes over it is saturated with moisture at body temperature (Fig. 1).
In centers where it is available, a saturation monitor can be used to adjust the air: oxygen mix to maintain saturations of 92 to 98% in the baby, and minimize the risk of oxygen toxicity. We have used different flow rates of oxygen and air and measured the resultant oxygen concentration using a MiniOX 111 oxygen meter. The readings were taken three times and the mean values are reported. The resultant table can help guide adjustment of flow rates to deliver the desired oxygen concentration. This is similar to the theoretical values achieved which are also shown in the table. For the theoretical calculations we assumed partial pressure of humidity saturated at 37ºC is 47 mm of Hg or approximately 5% of the total atmospheric pressure at sea level. The oxygen concentration is given by the formula: Final O2 concentration = n–n×5/100 where n is the oxygen concentration before saturation with humidity. Results Table I shows the oxygen mix when the total flow rate is 8 liters /minute and the ratio of air and oxygen is varied. The use of a humidifier reduces the oxygen concentration from 1% to 5% as shown in the Table. Table I Saturations of Oxygen Achieved with Different Flow Rates for Oxygen and Air
Discussion CPAP helps maintain the functional residual capacity (FRC) of infants, prevents atelectasis, augments surfactant production, reduces fatigue in ventilatory muscles, provides respiratory stimulation against apnea and allows gas exchange(11). Oxygen is ideally used only in neonates who are continuously monitored. The flow mix of oxygen and air can be adjusted to keep the saturation around 96%. However in areas where saturation monitors are not available, bubbling air for CPAP would be safe. Bubbling CPAP has been found safe to be used by nurses(2). Use of the table provided in this study will help users to determine the quantities of oxygen being delivered to the child. A single prong CPAP, using a cut down endotracheal tube, or a large bore suction tube may be used. This has shown to be as comfortable for the baby as the more expensive nasal prongs(12). This is a cheaper alternative to nasal prongs. Mouth closure is not considered essential although it can raise pharyngeal pressure(13). The authors have utilized this system within their neonatal unit for the last 10 years both for neonates with respiratory distress prior to ventilation (with a view to reduce the need for mechanical positive pressure ventilation) and also for weaning from the ventilator. A commercial version of the CPAP system is available in the market for Rs 155,000. All elements of the system described here can be bought for Rs 500 ($10) except the humidifier which is available for Rs 4500 ($100). Widespread use of this system has the potential for saving lives in small hospitals where there is no facility for mechanical ventilation of babies. Contributors: RSB and JP conceived the project, CK and AS did the measurements. All authors contributed to the manuscript preparation. JP will be guarantor. Funding: None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
![]()