|
|
Review Article Indian Pediatrics 2008; 45:285-294 |
||||||||||||||||||||||||||||
|
Hypotension in Preterm Infants |
||||||||||||||||||||||||||||
|
Liverpool Women’s Hospital, Crown Street, Liverpool,
United Kingdom L8 7SS.
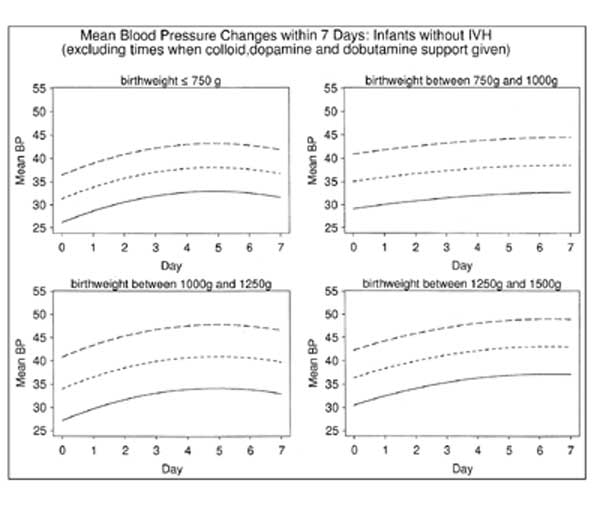
Introduction Hypotension occurs frequently in preterm neonates in the intensive care unit(1,2). Hypotension is reported to occur between 16 to 52% of preterm infants(1,3). The recognition and treatment of hypotension in the preterm infants are important because of the potential for adverse short and long term prognoses. Definition of Hypotension in Preterm Neonates Blood pressure in preterm infants can be measured both invasively, using intra-arterial catheters and non-invasively. Invasive blood pressure measurement is the gold standard(4,5). In hypotensive newborns non-invasive measurements tend to over-estimate blood pressure(6). Invasive pressure monitoring has it’s problems too. The pressure reading is affected by the mechanical properties of the intra-arterial catheter and the transducer system and presence of air bubbles. The above factors cause excessive damping leading to low systolic and high diastolic readings(4,5). Mean blood pressure is less affected by these and hence reliable even in the presence of a damped trace(5). ‘Normal’ blood pressure should be defined as the pressure, which ensures adequate organ perfusion(1, 8). The normal values will depend on gestational age, birthweight and postnatal age. Many studies have attempted to establish normal blood pressure ranges for very low birth weight (VLBW) infants. Most of the studies have drawbacks of having retrospective data, small number of infants, infrequent blood pressure measurements, inclusion of infants on inotropes and those with cerebral injury(2,5,9). Cunningham, et al.(10) have analyzed computerized data on a large cohort of patients over a 5-year period. After removing artifacts, excluding children with IVH and those on inotropic support they have published normative data for the first seven days of life in VLBW infants. They defined hypotension as less than the 10th centile for birth weight and postnatal age. This is a comprehensive dataset and probably serves as a useful reference range (Fig. 1).
Systemic hypotension in neonates may be associated with multiorgan injury and adverse long-term outcome. The association is not clear and the exact relationship and the rationale behind treating hypotension based on arbitrary cut off values is debatable(8). Blood Pressure and Cerebral Blood Flow Cerebral blood flow is one of the major determinants of oxygen delivery to the brain(1). The perfusion pressure in the cerebral arteries and vascular resistance determines cerebral blood flow. In older children and adults cerebral autoregulation maintains cerebral perfusion over a wide range of perfusion pressures(11). There has been conflicting evidence on the ability of hypotensive preterm infants to autoregulate(11-13,18). Lou, et al.(12) in a study on 16 neonates demonstrated a relationship between cerebral blood flow and blood pressure and concluded that autoregulation may be lost in sick infants. In contrast, in a cross-sectional study of 27 preterm infants, Tyszczuk, et al.(13) failed to show any such correlation. They also examined the recommendations made by some authors that a blood pressure above 30mm of Hg should be maintained to prevent cerebral injury(14,15). The authors found no difference in cerebral perfusion between groups with mean arterial blood pressure above or below 30 mm of Hg. It appears that cerebral autoregulation is impaired to a certain extent in sick preterm infants and may be dependent on mean arterial blood pressure. But the minimum blood pressure required to maintain cerebral perfusion is unclear and the current treatment thresholds for hypotension suggested by various authors based on ‘normal’ blood pressure ranges are at best arbitrary. There is also evidence emerging that cardiac output rather than mean arterial blood pressure is a more important determinant of cerebral oxygen delivery(16). Hypotension and Cerebral Injury Periventricular hemorrhage: Periventricular hemorrhage is an important cause of long-term morbidity in preterm infants(17). Many studies have shown an association between low systemic blood pressure and intra-ventricular hemorrh-age(2,10,14,15). Miall-Allen, et al. demonstrated a significant relationship between a mean blood pressure of less than 30 mm of mercury and significant cerebral lesions in very low birthweight infants(14). Correlation between systemic hypo-tension and fluctuations of blood pressure with intraventricular hemorrhage has been found by other authors(2,10,15). In contrast to the above studies, Tyszczuk, et al.(13) failed to show any relationship between low blood pressure and cranial ultrasound abnormalities. It is possible that a statistical association between IVH and hypotension is not necessarily a causal relationship. Hypotension and periventricular hemorrhage may be common complications of preterm birth. Periventricular leukomalacia: Periventricular leukomalacia (PVL) is strongly associated with neurodevelopmental morbidity and cerebral palsy(18). The areas of the brain involved in periventricular leukomalacia fall in the watershed zones of the penetrating branches of the cerebral arteries and are vulnerable to disturbances in cerebral blood flow(19). Conditions with potential reduction in cerebral blood flow like hypocarbia and patent ductus arteriosus with shunting have been associated with PVL(20, 21). Maill Allen, et al.(14) found a higher incidence of severe abnormalities including cystic PVL in preterm neonates who had a mean blood pressure less than 30 mm Hg. Tsuji, et al.(18) found an approximately 50% incidence of cranial ultrasound abnormalities including PVL in preterm neonates with probable impaired cerebral auto-regulation(18). Both Cunningham, et al.(10) and Watkins(2) failed to show any consistent correlation with systemic hypotension and PVL. It is surprising that many of the epidemiological studies have failed to establish a link between hypotension and PVL, given the pathophysiology. Most of the preterm newborns have some element of auto-regulation and blood pressure is only one of the determinants of cerebral blood flow(11). Probably there is a distinct group of sick preterms in whom cerebral autoregulation may be impaired in whom low blood pressure may contribute to the pathogenesis of PVL(18). Pathophysiology of Hypotension in Preterm Infants Blood pressure is dependent on cardiac output and systemic vascular resistance. Cardiac output is determined by preload, myocardial contractility and afterload(22). The contribution of left ventricular output towards maintenance of blood pressure in very low birthweight infants is unclear. More than one researcher has found a normal or high ventricular output in hypotensive preterm infants(23,24). These babies often have a low systemic vascular resistance, often associated with a significant shunt across a PDA. Kluckow, et al.(25) found a weak correlation between left ventricular output and blood pressure in preterm infants after accounting for ductal shunting. Myocardial dysfunction may be a factor in preterm hypotension. Gill and Weindling in a study on 75 low birth weight infants found a myocardial dysfunction in approximately half of the hypotensive infants(26). But other studies have failed to show such an association(23,24). Low circulating volume does not seem to be a major contributor towards preterm hypotension. Management of Hypotension The treatment of neonatal hypotension should be based on an overall assessment of cardiovascular status of the infant and not blood pressure alone. The heart rate, peripheral perfusion and urine output should be considered in addition to blood pressure(1). An elevated lactate concentration on blood gas analysis indicates low tissue perfusion in the absence of metabolic diseases. The value of CVP monitoring in preterm newborns with systemic hypotension is uncertain, but serial measurements may guide use of volume expansion(1,27). Echocardiographic evaluation can serve as useful adjunct, but is not readily available in most neonatal units. Volume expansion: Assessment of circulating blood volume is difficult in the clinical setting. Even in the absence of hypovolemia, volume expansion may increase blood pressure through the Frank-Starling mechanism(1). But many studies strongly indicate that absolute hypovolemia is an infrequent cause of hypotension in the preterm infant(28). Bauer, et al.(29) in study on 43 preterm infants did not find a correlation between systolic blood pressure at normal blood volumes. Lundstrom, et al.(30) found that volume expansion increased cardiac output without any effect on blood pressure in preterm infants. Gill, et al.(31) in a randomised controlled trial comparing dopamine to volume expansion found dopamine to be more effective in improving blood pressure. The type of fluid to be used for volume expansion, again has been contentious. A randomised controlled trial has shown no benefit of human albumin solution in comparison to isotonic saline for volume expansion in hypotensive preterm infants(32). Kavvadia, et al.(33) in a study on different fluid regimens in ventilated infants found a higher incidence of adverse lung function in preterm babies who received more colloids. This probably was related to protein leak into the pulmonary interstitium. Concerns about association of increased mortality with the use of human albumin in adult intensive care patients have been refuted by a recent large randomized controlled trial(34,35). Considering the fact that human albumin solution is more expensive and there is a theoretical risk of blood-borne infections, it is prudent to use isotonic saline as a first line volume expander unless there is significant hypo-albuminemia. Overzealous administration of fluids to preterm infants may be harmful. Van Marter, et al.(36) in a case control study found an association between excessive fluid administration and broncho-pulmonary dysplasia. Greenough, et al.(37) demonstrated an increase incidence of adverse neurodevelopmental outcome in preterm newborns who received colloids for fluid resuscitation in the perinatal period. Given the fact that hypovolemia is infrequent in hypotensive preterm babies and the concerns raised regarding excessive fluid administration in the perinatal period, it would be prudent to recommend that no more than one fluid bolus between 10 and 20 mL/kg be used for treatment of hypotension unless there is evidence of significant fluid losses and/or hypovolemia(1). If there is no improvement with the above strategy the infant is likely to benefit from inotropes. Inotropes and vasopressors for treatment of hypotension: Inotropes and vasopressors have been used for treatment of hypotension in preterm infants routinely(1,38). The distribution and maturation of the receptors to these drugs may be gestation dependent and could explain the differences in cardiovascular responses at various gestational ages(38). Dopamine: Dopamine is an endogenous catecholamine precursor of noradrenaline. It exerts cardiovascular effects through its action on peripheral dopamine receptors (DA1 and DA2), a and b-adrenergic receptors and serotonin receptors(38). The dose-dependent actions of dopamine have traditionally been explained by its effect on the different receptors. At low doses (0.5- 2 mg/kg/min) action on dopaminergic receptors are thought to predominate leading to increased renal blood flow. At medium doses (2-6 mg/kg/min) stimulation of b-adrenergic receptors leads to increased cardiac rate and output with some peripheral vasodilatation. At higher doses a-adrenergic and serotonin receptor activation is more prominent leading to vasoconstriction and increase in systemic vascular resistance(38). But these dose dependent actions are not always seen in preterm infants. Plasma concentrations of dopamine are dependent on metabolism and clearance rather than infusion rates(39). Hepatic and renal dysfunction affects dopamine clearance further. Also the effects of dopamine may vary due to the gestational age dependent peculiarities of the catecholamine receptors(40). Though there is some evidence that dopamine exerts a vasodilatory effect on the renal vasculature, many recent studies have not shown this effect (41,42). Experimental and clinical studies indicate dopamine exerts its cardiovascular effects in a dose range of 2.5 to 20 mg/kg/min(31,43,44). Doses more than 20 µg/kg/min are generally avoided because of the possibility of alpha-receptor mediated vaso-constriction and fall in cardiac output(45). Persisting hypotension on dopamine at a dose of up to 20 µg/kg/min would be an indication for adding other inotropes. Dobutamine: Dobutamine is a synthetic catechol-amine analogue. Dobutamine exerts its cardio-vascular actions through direct stimulation of beta and alpha-adrenergic receptors(1,28,46). It is relatively beta-1 cardioselective with low affinity for peripheral alpha-1 and beta-2 receptors. Hence, it has a predominant inotropic effect with relatively less chronotropic and vasoconstrictive effects. Dobutamine administration is usually associated with variable drop in systemic vascular resistance (24,45,46). In adults it improves cardiac contractility, stroke volume and output with relatively little effect on blood pressure. Because of its modes of action, dobutamine is most likely to be beneficial in newborns with myocardial dysfunction and high peripheral vascular resistance(47). The dose range used in preterm neonates varies between 5-20 µg/kg/min(1,43-45,48). Most of the randomised controlled trials comparing dopamine to dobutamine for the treatment of hypotension in the preterm infants have concluded that dopamine is more effective in improving blood pressure in preterms(43-45,48). But dobutamine seems to be superior in improving cardiac output and systemic blood flow(45,48). A recent meta-analysis found no difference in outcomes apart from changes in blood pressure between the groups treated with either dopamine or dobutamine(49). Dopamine should be the first choice inotrope if short-term improvement in blood pressure is the goal. Dobutamine could be considered as a first line if there is documented myocardial dysfunction. Dobutamine has the advantage that it can be administered safely through peripheral veins compared to dopamine. Other catecholamines: The experience with adrenaline and noradrenaline in preterm infants is limited. There are some studies on their successful use in hypotension resistant to conventional inotropes in preterm infants(50,51). The use of adrenaline and noradrenaline could potentially cause intense vaso-constriction and organ injury. Corticosteroids: The clinical importance of the adrenal glands is well known(52). The commonly recognised cardio-vascular effect of adrenal steroids in humans is to increase blood pressure by the steroid (mineralocorticoid) induced retention of sodium and water. Steroids also enhance blood pressure by increasing vascular reactivity to other vasoactive substances. They up-regulate catecholamine receptors in the myocardium and peripheral blood vessels, increasing sensitivity to endogenous and administered catecholamines. They also enhance the activity of phenylethanolamine N-methyl transferase, the terminal enzyme in adrenaline synthesis in the adrenal glands. Other mechanisms proposed included inhibition of nitric oxide induced vasodilatation, inhibition of vasodilator prostanoids and upregulation of angiotensin II receptors(53). There is increasing evidence that sick preterm infants may have an absolute or relative cortisol deficiency(54). Korte, et al.(55) found low cortisol levels and impaired response to physiological dosed of ACTH in very low birth weight infants. They were able to discontinue pressor support in all the steroid- responsive infants between 28 to 54 hours from the start of treatment with steroids. Moise, et al.(56) in a retrospective analysis found that antenatal steroid administration resulted in less requirement for blood pressure support in premature infants between 23 to 27 weeks gestation. A recent randomised controlled study of prophylactic hydrocortisone in the first three hours of life in preterm infants, noted a significant reduction in the need for vasopressors during the first two days of life in the treated group(57). In small case series Helbock, et al.(58) and Ng, et al.(59) demonstrated cortisol deficiency in pressor-resistant hypotensive preterm infants with a good response to treatment with steroids. Bourchier and Weston in a randomized trial, found intravenous hydrocortisone, given over a six day period to be as effective as dopamine in the treatment of hypotension in VLBW infants(60). There was no difference in short-term outcomes. Long-term outcomes were not reported. Gaissmaier et al studied the effect of a single 250 mg/kg dose of dexamethasone in patients requiring adrenaline for treatment of hypotension(61). They were able to discontinue adrenaline at 12 hours in 5 of 8 infants in the dexamethasone group compared to 1 of 9 given placebo. Short-term outcomes did not differ. The potential side effect from steroid treatment include hyperglycemia, hypertension, gastro-intestinal hemorrhage, intestinal perforation, fluid retention, catabolic state, growth failure, increased rate of infections, hypertrophic cardiomyopathy, increased retinal blood flow and suppression of the hypothalamopitituary adrenal axis. Neither of the above studies demonstrated any major side effects attributable to steroid treatment apart from transient hypertension in a few infants. In summary steroids seem to be beneficial in treatment of hypotension in preterm infants unresponsive to maximal conventional doses of. The dose of hydrocortisone for preterm hypotension in published literature has varied from 1-6mg/kg for 4-6 hourly for durations varying from 5 days to 2 weeks in tapering doses(58-61). There are no differences in short-term outcomes evident from the small randomised trials. The long term outcomes in these groups of patients need to be addressed in larger trials. Due to the concerns regarding the long term neurodevelopmental outcome of preterm infants treated with steroids for chronic lung disease in the early neonatal period it would be prudent to use hydrocortisone only in hypotensive preterm infants resistant to conventional therapies(62). Other Agents: Excess synthesis of nitric oxide leading to activation of guanylate cyclase and increased levels of cyclic guanosine monophosphate has been implicated in septic shock. Methylene blue, a soluble guanylate cyclase inhibitor has been used successfully to treat septic shock in five neonates(63). Dopexamine is a relatively new synthetic catecholamine. It has been shown to improve blood pressure and urine output in neonates(64). Milrinone is a phosphodietserase inhibitor which may be useful in improving cardiac contractility and reducing afterload in subjects with cardiac dysfunction. A single study looking at the use of milrinone in preterm neonates has reported encouraging results(65). Arginine vasopressin has reported to improve cardiovascular function in a small number of newborns with vasodilatory shock following cardiopulmonary bypass(66). But there is very limited data on safety and efficacy of these newer drugs in preterm infants. Table I Drugs for Treatment of Hypotension in Neonates
Supportive Measures Hypotension should not be considered in isolation. The cause of hypotension needs to be considered and corrected. If there has been an acute bleed (commonly intraventricular), blood transfusion may be required. If there are electrolyte disturbances including blood sugar abnormalities, they need to be optimised. Acidosis desensitizes catecholamine receptors and needs to be corrected by either alkali infusions (bicarbonate or THAM) or optimising ventilation if the cause is respiratory. Hypoxia should be corrected by appropriate ventilatory management. High doses of sedatives and opioids used in ventilated infants can cause hypotension and may need to be reduced. Summary and Conclusions Hypotension occurs frequently in preterm infants on intensive care. The importance of hypotension lies in the presumed effect of blood pressure variations on cerebral blood flow apart from other organ perfusion. Though majority of the hypotensive infants are not hypovolemic, a fluid bolus could potentially improve cardiac output. Infants who are hypotensive despite volume expansion require inotropic support. Dopamine seems more effective than dobutamine in improving blood pressure. Experience with other inotropes is limited. Steroids may be used in hypotension refractory to high doses of ionotropes. Other physiological parameters need to be optimised along with pharmacological and fluid management of hypotension. Funding: None. Competing interests: None stated.
|
![]()