|
|
Research Papers Indian Pediatrics 2008; 45:279-284 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Evaluation of the Role of Ultrasonography in Diagnosis of Autoimmune Thyroiditis in Goitrous Children |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
R K Marwaha, N Tandon*, Ratnesh Kanwar*, M Ashraf Ganie, V Bhattacharya, DHK Reddy*, Sripathy Gopalakrishnan, R Aggarwal, Khushi Grewal, SK Ganguly and Kalaivani Mani# From the Department of Endocrinology and Thyroid
Research Center, Institute of Nuclear Medicine and Allied Sciences,
Timarpur, Delhi 110 054 and Departments of *Endocrinology and
#Biostatistics, All India Institute of Medical Sciences, Correspondence to: R K Marwaha, Department of
Endocrinology and Thyroid Research Center, Manuscript received: May 25, 2007; Initial review
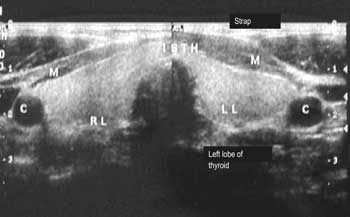
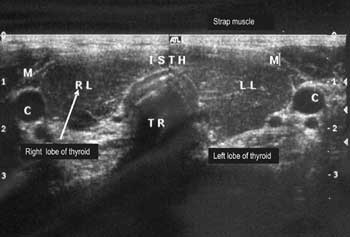
completed: July 11, 2007; Abstract To evaluate the role of thyroid ultrasound in children with autoimmune thyroiditis diagnosed either on cytopathology or by the presence of thyroid peroxidase antibodies. Design and Settings: Children presenting for the first time to the Thyroid Clinic at the Institute of Nuclear Medicine and Allied Sciences for the complaint of goiter over a two year period (January 2005-December 2006) were studied. Subjects: 695 school children (244 boys and 451 girls) aged 5-18 year were studied. Methods: Children were subjected to thyroid ultrasound, cytopathology, thyroid peroxidase antibody and thyroid function tests. Results: Overall, 16% of goitrous children had hypoechogenicity on ultrasound, 15.2% had cytopathological evidence of thyroiditis, 10.6% had positive thyroid peroxidase antibodies and 25.2% had abnormal thyroid function tests. Subjects with hypoechogenicity had higher percentage of thyroiditis on cytopathology (41.4% vs. 10.3%; P<0.01), thyroid peroxidase antibody positivity (30.6% vs. 6.8%; P<0.01) and thyroid dysfunction (46.8% vs. 21.2%; P<0.01) than those with normal echogenicity. Conclusion: Thyroid USG has a useful, though limited, role in excluding thyroid disease in children. The sensitivity of echogenicity for the diagnosis of autoimmune thyroiditis in children is less than that reported in adults. Key words: Anti-TPO antibodies; Autoimmune thyroiditis; Fine needle aspiration cytology; Thyroid dysfunction; Thyroid ultrasound. Introduction In the diagnosis of autoimmune thyroiditis (AT), though fine needle aspiration cytology (FNAC) is regarded as the gold standard, its invasive nature and difficulty in performing the procedure on small goiters particularly in children precludes its use in clinical practice routinely. Thus, the diagnosis of autoimmune thyroiditis is generally based on the identification of elevated thyroid peroxidase antibody (TPO Ab) levels. However, this approach is liable to miss some cases because not all patients with AT have elevated TPO(1,2). Ultrasonography (USG) has proved to be a useful tool in the evaluation of adults with thyroid diseases(3-5). Reduced echogenicity on USG is considered to be characteristic of AT(6). In adults, USG thyroid has been shown to have a definite value in the diagnosis of autoimmune thyroiditis. The degree of hypoechogenicity was not only found to have a significant correlation with the levels of circulating thyroid antibodies and thyroid dysfunction but was also shown to predict the evolution towards hypothyroidism in euthyroid subjects(7). However, the role of USG in the evaluation of juvenile autoimmune thyroiditis (JAT) is not yet defined. The objectives of the present study were to identify the role of USG in the diagnosis of JAT and to evaluate its relationship with FNAC and thyroid antibody status in 5-18 year old children. Methods The study was conducted in 5-18 year old school children who presented with goiter, for the first time to the Thyroid Clinic at Institute of Nuclear Medicine and Allied Sciences (INMAS), between 2005-2006. None of the subjects were receiving either thyroxine or any other drug known to interfere with thyroid function at the time of evaluation. Patients with known thyroid disease were excluded. Informed consent was taken from the parents of all the children studied. The study protocol was approved by the ethics committee of INMAS. Ultrasonography of thyroid gland was performed with subjects in supine position and neck in hyper-extended position by a single sonologist (SKG) who was blinded to the clinical and biochemical status of the subjects, using a portable ultrasound machine (Aloka SSD-500, Tokyo, Japan) with a 7.5 MHz transducer. The gain settings of the ultrasound scanner were adjusted so that the lumina of the carotid artery and internal jugular vein were free of echoes. Hypoechogenicity was diagnosed if echogenicity of the thyroid was uniformly less than that of the connective tissue and similar to or less than that of the neck muscles (Fig. 1). Mild hypoechogenicity was defined when the echogenicity was less than that of connective tissue but more than that of strap muscles of the neck(8).
In addition to the detailed history and physical examination, these children were subjected to blood sampling for estimation of thyroid function status (free T4, free T3 and TSH), and thyroid peroxidase autoantibody (TPO Ab). FT3 and FT4 were analysed by radioimmunoassay (Immunotech, Beckman Coulter). Normal range for FT4, FT3 and TSH were 11.5–23.0 pM/L, 2.5–5.8 pM/L and 0.17–5.2 mIU/L respectively. The presence of either sub-clinical or overt hypo- or hyperthyroidism was used to define thyroid dysfunction. Anti TPO antibodies were analysed by electro-chemiluminescence assay (Cobas-Roche Elecys 1010 analyser). The range of measurement is 5-600 IU/mL. Values>34 IU/mL were defined as TPO Ab positive. The intra assay CV was <4.2% and inter assay CV <9.2 %. The analytical sensitivity was <5 IU/mL. Fine needle aspiration cytology (FNAC) was performed under aseptic conditions by using a 23-gauge needle as previously described(2). Statistical analysis: SPSS 10.0 version was used to analyze the data. In addition to descriptive statistics, the percentage of subjects positive or negative on particular test modality, were compared by Students ‘t’ test. Diagnostic accuracy of thyroid ultrasound was evaluated in terms of sensitivity (proportion of subjects with CLT who have an abnormal echogenicity), specificity (proportion of subjects without CLT who have normal echogenicity), positive predictive value, negative predictive value and misclassification rate. The diagnostic modalities were compared with each other alone and in various combinations to find the odds of identifying JAT. Results Among a total of 695 subjects studied, 244 (35.1%) were boys and 451 (64.9%) were girls. The descriptive analysis of all these subjects is shown in Table I. Overall, 16% of subjects had hypo-echogenicity on USG, 15.2% subjects had CLT on FNAC, 10.6% were TPOAb positive and 25.2% had abnormal thyroid function tests. Table I Descriptive Characteristics of the Children Studied
USG=ultrasound; TPO=thyroid peroxidase; FNAC=fine needle aspiration cytology; CLT=chronic lymphocytic thyroiditis; NST/FST=non specific/focal thyroiditis.
Subjects with hypoechogenicity had significantly higher percentage of CLT on FNAC than those with normal echogenicity (41.4% vs. 10.3%; P<0.01) (Table II). Similarly, USG hypoechogenicity was observed in 43.4% of subjects with CLT on FNAC, as compared with 11.04% of subjects without CLT (P<0.0001). Even among patients with a cytopathological diagnosis of colloid goiter, hypoechogenicity was observed in 10.3%. The likelihood of having FNAC proven CLT was 6.2-fold more (95% CI; 3.9-9.8; P<0.05) in glands with hypoechogenicity compared with subjects with normal echogenicity on USG. The sensitivity and specificity of USG hypoechogenicity if FNAC is considered as gold standard was 43.4% and 88.9% respectively. Positive predictive value (PPV) of USG with regards to the diagnosis of CLT on FNAC is 41.4% and the negative predictive value (NPV) was 89.7 %. Table II Prevalence of Cytopathological Chronic Lymphocytic Thyroiditis, TPO Antibody Positivity and Thyroid Dysfunction in Subjects with Normal Echogenicity and Hypoechogenicity on Thyroid Ultrasound
CLT = chronic lymphocytic thyroiditis; FNAC = fine needle aspiration cytology; Thyroid dysfunction = combination of sub-clinical or overt hypo- or hyperthyroidism; * The prevalence of CLT, TPO Ab positivity and thyroid dysfunction or any combination of these was significantly more in subjects with hypoechogenicity compared with those with normal echogenicitiy. Subjects with hypoechogenicity had a significantly higher prevalence of TPOAb positivity than subjects with normal echogenicity (30.6% vs. 6.8%; P<0.01) (Table II). Similarly, USG hypoechogenicity was observed in 45.95% of subjects with TPO Ab positivity, as compared with 12.4% of TPO Ab negative subjects (P<0.0001). The likelihood of TPO Ab positivity was 6.0 times more (95% CI; 3.6-10.1; P<0.05) in subjects with hypoechogenicity on thyroid USG. The sensitivity and specificity of USG hypoechogenicity if the diagnosis of JAT is based on TPO Ab positivity was 45.9 % and 87.6% respectively. PPV of reduced thyroid echogenicity as an indicator of thyroid autoimmunity as defined by TPO Ab positivity was 39.6% and the NPV was 93.2%. The sensitivity and specificity of USG hypoechogenicity, if the diagnosis of JAT is based on either CLT on FNAC or TPO Ab positivity, is 41.2% and 90.2% respectively. PPV and NPV of USG hypoechogenicity if the diagnosis of JAT is based on the above criteria is 49.5% and 86.3% respectively. The prevalence of thyroid dysfunction in subjects with hypoechogenicity on thyroid USG (46.8%) was significantly more than that in individuals with normal thyroid echogenicity (21.8%; P<0.01) (Table II). The mean TSH in subjects with a normal USG echogenicity (3.94±5.26 mIU/L) was significantly less than the TSH in subjects with USG hypoechogenicity (7.82±11.42 mIU/L). The sensitivity and specificity of USG to predict thyroid dys-function was 29.5% and 88.6%, respectively. PPV of USG for thyroid dysfunction was 46.8 %, while the NPV was 78.8 %. In comparison, the prevalence of thyroid dysfunction in individuals with CLT on FNAC or TPO Ab positivity was 47% and 51.4% respectively. The group with least prevalence of thyroid dysfunction comprised of subjects, who in addition to having normal echogenicity on thyroid USG had no evidence of CLT on FNAC and were also TPO Ab negative (Table III). TABLE III Percentage of Thyroid Dysfunction Among Different Tests
TPO– thyroid peroxidase; FNAC–fine needle aspiration cytology; USG–ultrasound; * This category includes individuals with hypoechogenicity on thyroid USG who may also have CLT on FNAC and / or TPO Ab positivity; # This category includes individuals with hypoechogenicity on thyroid USG who did not have CLT on FNAC and were TPO Ab negative. Discussion A diffuse reduction in thyroid echogenicity has been reported in 19-95% of adult patients with autoimmune thyroid disease. However, there is scant literature with regard to ultrasonography findings in children with autoimmune thyroiditis. The present study was designed to evaluate the role of thyroid echogenicity in diagnosis of thyroid autoimmunity in children. In the present study, the sensitivity and specificity of USG for the diagnosis of CLT on FNAC was 43.4% and 88.96% respectively. In adults, the sensitivity of USG has been reported to be 18.5%-95.1% and the specificity to be 96%- 100%(7-10). These differences could be due to difference in the population studied, differences in the stage of thyroid disease and also to differing methods in the assessment of thyroid echogenicity. In contrast to adults, we did not find any comparable study conducted in children. However, Ivarsson, et al.(11) noted that all 10 children with CLT on FNAC were hypoechoic on USG (sensitivity 100%), but the sample size was small. The same author reported that all subjects with diffuse colloid goiter had normal echo pattern on ultrasound. In contrast we found that 10.3% of subjects with colloid goiter also had reduced thyroid echogenicity. In our study, 46% TPO Ab positive children had reduced echogenicity. A smaller study conducted in children noted that 12/14 (86%) subjects positive for TPOab had hypoechogenicity(12). However, a similar study in adults noted that 68% of TGAb positive and TPO Ab positive subjects were associated with hypoechogenicity on thyroid ultrasound(13). A significant correlation between ultrasound echogenicity by grey scale analysis and TPO Ab was reported by Mazziotti, et al.(14), but the same findings were not confirmed in a subsequent study(15). In the present study, the sensitivity and specificity of USG hypoechogenicity in predicting abnormal thyroid function status was 29.5% and 88.6%, respectively. In adults, thyroid hypoechogenicity has been reported to have a higher sensitivity than TPO Ab positivity (100 vs. 63.3%) for diagnosing or predicting thyroid dysfunction(5). In another study conducted in adults, positive predictive value of grade 2-3 pattern of hypoechogenicity for detection of autoimmune thyroiditis ranged from 85-94%(9). Our study showed that among subjects with hypoechogenicity, 41% had CLT on FNAC, 30.6% had positive TPO Ab and 46.8% had abnormal thyroid function. Pederson, et al.(8) have noted that, among adult cases with reduced thyroid echogenicity, 79% had CLT, 67% had TPO Ab positivity and 64% had abnormal thyroid function tests. In the study by Marcocci, et al.(7) hypothyroidism was seen in 45.5% of subjects with hypoechogenicity. A comparison of various tests in predicting thyroid dysfunction shows that individuals with normal echogenicity, negative for TPO Ab and with no evidence of CLT on FNAC, had less than 20% likelihood of thyroid dys-function. In summary, thyroid USG has a useful, though limited, role in excluding thyroid disease. The sensitivity of echogenicity for the diagnosis of autoimmune thyroiditis in children is less than that reported in adults. This could possibly be because, in adults the autoimmune process is well established, whereas it is still in the process of evolution in children. Prospective studies in children with thyroid hypoechogenicity will be useful to assess the value of this investigation in predicting future thyroid dysfunction. Acknowledgments The assistance provided by the following team members is gratefully acknowledged: H R Singha, Sushma Tripathi, Harish Chandra, M Pillai, Jagat Singh, Kuntal Bhadra. Contributions: RKM and NT were involved with the planning, collection of data, analysis and writing. RK, RA, KG, SG were involved in collection of data. MAG, DHKR were involved in design and analysis. VB was involved in cytopathological evaluation. SKG was involved in performing thyroid ultrasound. KM contributed to design and statistical analysis. Funding source: This study was supported by a research grant from the Defence Research and Development Organization, Ministry of Defence, Government of India. Competing interest: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()