|
|
Research Papers Indian Pediatrics 2008; 45:271-277 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
BCG Reaction in Twin Newborns: Effect of Zygosity and Chorionicity |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
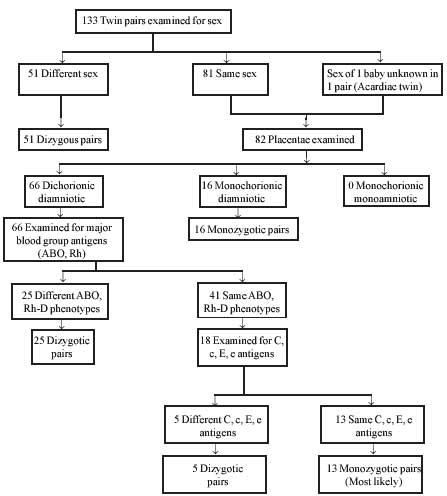
Introduction BCG is a live attenuated vaccine given routinely to all newborns in India under the Universal Immunization Program(1). It is an important part of armamentarium for prevention of serious tuberculosis in children(2-7). BCG induces delayed type of hypersensitivity reaction and cell mediated immunity in the host 4-8 weeks after the vaccination. A sequence of changes has been described at the site of BCG vaccination in the form of papule, pustule, ulcer and scab after 4 to 12 weeks which culminates in scar formation and is considered an evidence of successful vaccination(1,4,7). All stages of scar formation may be seen at 12 weeks after BCG vaccination in both low birth weight (LBW) and normal birth weight babies(8) and scar formation may take six months or even longer(9). Several studies showing significantly higher concordance of tuberculosis among monozygotic (MZ) than dizygotic (DZ) twins have provided a strong support for genetically determined susceptibility to tuberculosis(10,11). It is of interest to understand the inheritance of measurable immune responses in humans exposed to controlled challenges with mycobacteria, such as immunization with Bacillus-Calmette-Guerin (BCG) vaccine. We conducted this study to find out the local response to BCG vaccination in twin newborns after 14 weeks and whether it was modified by chorionicity and zygosity. Methods This prospective study was conducted in a tertiary care hospital of Delhi after obtaining permission from the Ethical Committee of the institution. An informed consent was taken from the parents before subject enrolment. All twins delivered during the study period from February to September 2005 were assessed for chorionicity by gross and histopathological examination of placentae. Zygosity was determined on the basis of phenotypic sex, placental morphology and 7 blood group phenotypes (ABO, Rh-D, Rh-C, Rh-c, Rh-E and Rh-e) in 110 twins (Fig. 1).
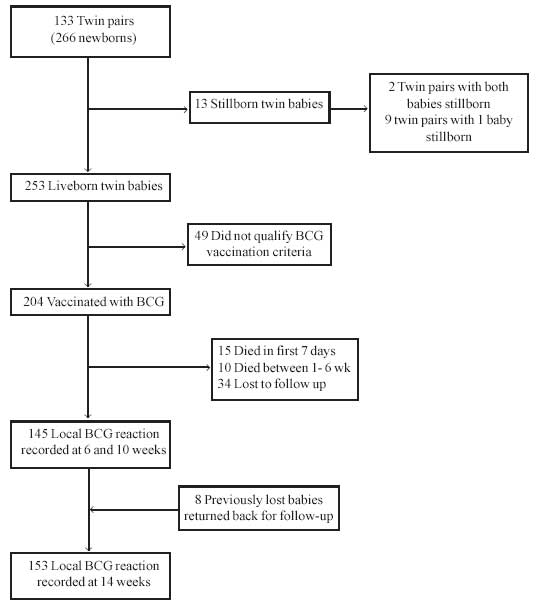
All twin babies born at ³33 weeks of gestation with birth weight ³1500 g were administered 0.1 mL of BCG within 48 hours of life by two trained staff nurses who had more than 10 years experience in the immunization clinic. Same BCG vaccine batch (Danish 1331 strain; BCG Laboratory, Guindy, Chennai) was used for each sibling pair. The freeze dried vaccine was reconstituted with normal saline and given intradermally on the left arm just above the insertion of the deltoid muscle with a 26 Gauge needle and tuberculin syringe to produce a wheal of 5 mm. The left over reconstituted vaccine was discarded after 3 hours. All cold chain precautions were taken. Simultaneously, OPV and hepatitis-B vaccine were also administered in these babies as per Delhi State Immunization Schedule. All the newborns received hospital care in either neonatal intensive care unit or postnatal ward as per the unit protocol. At the time of discharge, the parents were counseled about exclusive breast-feeding, immunization and regular follow-up visits. Three follow-ups were done at 6(+1), 10 (+1) and 14(+1) weeks after BCG vaccination to record the local reaction at the vaccination site in the form of no reaction (baby did not show any stage of BCG reaction during entire 14 week follow-up), abortive reaction (baby initially developed papule/pustule at the vaccination site that disappeared without scar formation by 14th week)(8), papule, pustule, ulcer, scab or scar. The primary outcome measure of BCG uptake was the presence of local response, in any form, after 14 weeks of vaccination. All the responses at the site of BCG vaccination were recorded by the same observer (PG). After 14 weeks, if there was an abortive reaction or no local reaction, Mantoux test was done to document development of delayed type hyper-sensitivity to BCG immunization. Mantoux testing was done with SPAN’s tuberculin PPD (Span Diagnostics Ltd., Surat, India), Code No. 18411 (5TU PPD/0.1 mL). Source material was calibrated against batch RT-23 manufactured by Statens Serum Institute, Denmark. A 0.1 mL of tuberculin PPD solution was drawn into a sterile tuberculin syringe fitted with a short 26 Gauge needle. PPD was injected intradermally on the flexor surface of left forearm about 3-4 inches below the elbow joint, by inserting the tip of the needle into the most superficial layers of the skin with the needle bevel pointing upwards. Results of the Mantoux test were read between 48-72 hours by ball-point pen technique(12). Infants showing transverse induration ³5 mm were considered ‘Mantoux converted’ after BCG vaccination. Qualitative data of local response to BCG vaccination was compiled and analysed by SPSS/PC Version 13.0 software using descriptive statistics, Cohen’s Kappa and Z-test. Results A total of 133 pairs of twins were delivered during the study period. Based on placental examination, there were 117 dichorionic and 16 monochorionic twin pairs. Zygosity was determined in 110 twin pairs out of whom 29 pairs were monozygotic and 81 were dizygotic. A total of 204 twin babies received BCG vaccination (Fig. 2). Mean (SD) period of gestation was 30.6 (1.6) weeks and mean (SD) birth weight was 2074.3 (342.7) grams. At 6 weeks, local BCG reaction was studied in 145 twin babies (Fig. 2). There was no reaction in 44.1% babies; a papule was observed in 46.2% of the babies, whereas a pustule was present in 9.7% infants (Table I). TABLE I Local BCG Reaction in Twins
*No case had scab in any of the groups. At second follow-up after 10 weeks of BCG vaccination, 20% (n=29) twin babies did not show any local reaction at the site of vaccination (Table I). At 14 weeks after BCG vaccination, scar formed in 63 (41.2%) of 153 babies who came for follow up (Fig. 2). Overall, 25 (16.3%) twin babies did not show any local reaction at the site of vaccination. (Table I).
Of 25 babies, who did not show any local reaction at 14 weeks of follow-up, there were 20 ‘true non-reactors’ (who did not show any stage of BCG reaction during entire 14 week follow-up). Among them, no one had Mantoux conversion also. Five (2.8%) ‘abortive reactors’ (who showed papule/pustule initially that disappeared without scar formation by 14th week) were seen. Concordance was seen in two pairs (1 MZ and 1 DZ) in which both babies showed ‘abortive reaction’. Third pair (MZ) showing ‘abortive reaction’ was discordant i.e., only 1 baby of that pair had ‘abortive reaction’. There was Mantoux conversion in 1 (20%) of the ‘abortive reactors’. Intra-pair measure of agreement in monozygotic group was highly significant at all stages of follow-up (P<0.01). Similarly, intra-pair measure of agreement was highly significant in dizygotic group also (P<0.01). When Cohen’s Kappa values of the two groups were compared by Z-test, the monozygotic intra-pair agreement was not significantly larger than the dizygotic intrapair agreement (Table II). TABLE II Intra-Pair Measure of Agreement for Response to BCG Vaccination in Monozygotic and Dizygotic Pairs
n=number of pairs in which both babies of the pair survived and turned up for follow-up No significant difference between Kappa values of the two groups (Z-test) (P>0.05). Intra-pair measure of agreement for local BCG reaction was significant in both monochorionic and dichorionic group of twins at all stages of follow-up (P<0.01). After applying Z-test, no significant difference was appreciated in the intra-pair agreement for local response to BCG reaction between monochorionic and dichorionic twins (Table III). TABLE III Intra-Pair Measure of Agreement for Response to BCG Vaccination to Monochorionic and Dichorionic Pairs
n=number of pairs in which both babies of the pair survived and turned up for follow-up. No significant difference between kappa values of the two groups (Z-test) (P>0.05). Discussion In the present study, the sequence of BCG scar evolution was found to be similar to that reported in singletons(8). A papule formed at the BCG vaccination site as early as 6 weeks in 46.2% of the twin babies and got transformed into pustule, ulcer and scar eventually. After 14 weeks of BCG vaccination, scar formed in 41.2% twin babies. Lower rate of scar formation may be explained by the hypothesis that twins being more frequently preterm and low birth weight may have immunological immaturity at birth and may behave in the similar manner as LBW singletons do with BCG vaccination(8). Thayyil-Sudhan, et al.(13) reported that 90% of preterm babies vaccinated at 34-35 weeks of post conceptional age developed scar after 6-8 weeks of vaccination. Though scar formed in only 41.2% babies after 14 weeks, yet 42.5% of twin infants had pre scar stages of local BCG reaction. Thus a total of 83.7% twins developed local BCG reaction. Similar observations had been made previously in LBW singletons(8). Aggarwal(9) also recorded that 33.2% infants had a papule or pustule even after 6 months and scar developed in 65% and 94.2% infants at 10-12 weeks and 6 months respectively. In our twin babies also, it was hoped that scar would eventually form. This is an important observation that pre-scar stages may be present even at 14 weeks and scar formation may take longer time. In the present study, there were 20 ‘true non-reactors’ who did not show any stage of BCG reaction during 14 weeks follow-up. None of these babies had Mantoux conversion as well, indicating that BCG vaccination might have failed in them. Five ‘abortive reactors’ were also seen. A positive PPD reaction was found in one abortive reactor after Mantoux test which indicated that BCG was taken up. Other tests of cell mediated immunity like leucocyte migration inhibition have been documented to be positive in babies with scar failure(14). Therefore, a twin baby showing abortive reaction may not require a repeat BCG vaccination. In the present report, BCG response showed a significant degree of intra-pair agreement in both monozygotic/dizygotic and monochorionic/dichorionic twins (P<0.01). However, monozygotic twin intra-pair agreement was not significantly greater than that of dizygotic twins. These results reveal that local response to newborn BCG immunization in humans is regulated by a mechanism capable of producing similar responses in monozygous and dizygous twins. Similarly, monochorionic twin intrapair measure of agreement was not significantly greater than that of dichorionic twins. These results are in consonance with those of Sepulveda, et al.(15). Their study population consisted of 17 monozygotic and 18 dizygotic twin pairs. All had a BCG scar and were tuberculin tested at 3-34 months of age. Both twin pair correlations in adjusted tuberculin reactivity were significantly greater than zero (P<0.01) and led to a heritability estimate of 0.28. However, the monozygotic twin correlation was not significantly larger than the dizygotic twin correlation, so that heritability was poorly estimated. In another study, Sepulveda, et al.(16) reported that concordance in BCG or tuberculin reactivity may not be related to the HLA molecules(15,16). In the present study also, the strong intra-pair agreement for local BCG reaction among monozygotic and dizygotic, as well as monochorionic and dichorionic twins further strengthen this hypothesis. The limitation of the study was that detailed genetic assessment including HLA typing of the twins was not done and comparison of local BCG reaction with singleton group of similar weight and gestation was not carried out; conclusions are thus based on historical data and reports. Contributors: MMAF conceptualized and designed the study, interpreted data, revised manuscript and approved the final version to be published. He will act as guarantor of the study. PG acquired data, drafted the article and helped in final approval of the manuscript. DS analysed the data, revised contents and helped in final approval. GD helped in interpretation of chorionicity and zygosity, revised the manuscript and helped in final approval. Funding: None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()