|
|
Case Reports Indian Pediatrics 2006; 43:357-360 |
||||
|
Constitutional Tetrasomy 18p |
||||
|
From the Cell Biology Division, Department of Cancer
Biology, The Gujarat Cancer & Research Institute, NCH Campus, Asarwa,
Ahmedabad 380 016, India and *MetaSystems, Correspondence to: Dr. Sonal R. Bakshi, Jr. Scientific
Officer, Cell Biology Division, The Gujarat Cancer & Research Institute,
NCH campus, Asarwa, Ahmedabad 380 016, India.
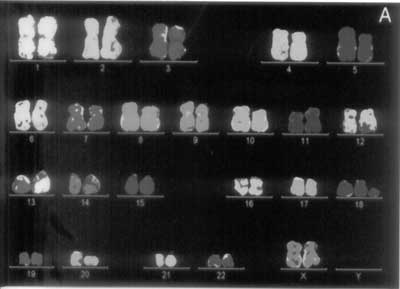
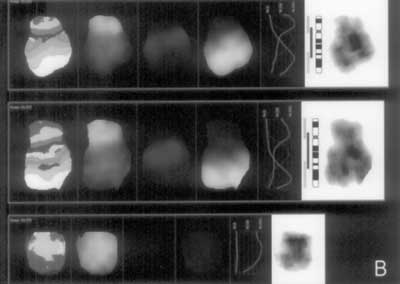
Chromosome analysis is indicated for conditions like mental retardation, dysmorphic features etc. Within the limits of conventional cytogenetics, various gross chromosomal anomalies are identified. In addition to this, other cryptic and rare constitutional chromosome anomalies are also increasingly uncovered with molecular cytogenetic techniques since the last decade. A patient with dysmorphic features and delayed development was referred to our laboratory for chromosomal analysis. Tetrasomy of 18p was established with the help of molecular cytogenetics. We wanted to study extended family members with a history of mental retardation to see if similar chromosomal marker was involved. Case Report An 8-month-old female child was referred for chromosomal analysis due to suspected congenital anomaly. The age of the parents at the time of patients’ birth were 30 and 32 years for mother and father respectively. The ultrasonography during pregnancy was normal. Her length, weight and head circumference were within the normal limits. Her urine analysis for reducing substance was normal and FeCl3 test was normal. The results of ultrasonography and fundus examination were also normal. There was no weight gain until the age of 6 months, however, later it was normal. Clinical examination revealed several dysmorphic features. With reference to the percentage of patients with one of 50 different phenotypic features listed in table on the website(1), the presence of the features in index patient was recorded. These features included, develop-mental delay, low set ears, small head, high arched palate, small mouth and chin, epicanthic folds, crossed eyes, long philtrum, down-slanting eyes, asymmetric face, hyper telorism, and hypotonia. Her family history was remarkable with four cases of mental retardation from paternal side. The paternal aunt, 36/F is mentally retarded (IQ 60) having schizophrenia, dysmorphic features and short stature. Other relatives from previous generations, 40/F, 42/M are siblings with low IQ / mild mental retardation and socially less developed, the male relative is married, with no children. Another relative, a 16/F also has mental retardation. Karyotypic analysis of above mentioned four affected relatives, and normal individuals i.e. parents, a sibling, and paternal grandfather was normal. Conventional cytogenetic studies were carried out as per standard methods. M-FISH and M-BAND were carried out as per manufacturer protocol (Metasystems, Germany) at Germany. Based on the results of detailed cytogenetic analysis, the condition was diagnosed as tetrasomy of 18p (Fig. 1a and 1b), a known condition from the western countries, but reported for the first time from India. The family is registered on the web site(1) and useful literature was made available to the mother after translation in local language.
Discussion In order to arrive at an accurate diagnosis of genetic condition, the conventional cytogenetics needs to be substantiated with molecular methods. Use of m-FISH and m-BAND could simultaneously determine the origin and copy number of the chromosomal fragment in the marker i.e., tetrasomy of 18p. Use of multiplex fluorescent PCR has been reported previously, which gives additional information regarding parental origin of the marker(2). Both paternal(3), and maternal(2,4) origin has been reported. The abnormality of chromosome 18 is either inherited(5) or de novo(6,7). Pooling the data helps learn about genotype / phenotype correlations and aid in the recognition and diagnosis of tetrasomy 18p. Even in a relatively well-defined condition like Down syndrome, intrinsic variability of the phenotype has been observed. Similarly, tetrasomy 18p seems to display marked variability of phenotypic characteristics. However, combining certain common characteristics may point to a unique picture of an individual with tetrasomy 18p; as a firm definition of the phenotype of tetrasomy 18p has not been reached unlike Down syndrome. It is important to put on record such rare cases of genetic conditions, as there are relatively small numbers of cases in such category of chromo-some anomalies that provides opportunity to explore the mechanisms of anomalies that may be generalizable to other conditions. This is the first report of constitutional tetrasomy
18p from India. Laboratories dealing with clinical cytogenetics are
meager in India compared to the western countries, and rarely equipped
with molecular cytogenetics facilities. This fact may have masked the
real incidence of many subtle chromosomal abnormalities. | ||||
|
References | ||||
|
|
![]()