|
|
Brief Reports Indian Pediatrics 2006;43:344-348 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Profile of Neonates Admitted in Pediatric ICU and Validation of Score for Neonatal Acute Physiology (SNAP) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Anil Vasudevan, Atul Malhotra, Rakesh Lodha and S.K. Kabra From the Department of Pediatrics, All India Institute
of Medical Science, Ansari Nagar, Correspondence to: Rakesh Lodha, Assistant
Professor, Department of Pediatrics, Manuscript received: January 4, 2005, Initial review
completed: March 4, 2005;
Pediatric and neonatal intensive care are emerging specialties in India. Many hospitals in India treat newborns in pediatric ICUs (PICU). The profile of neonates admitted in PICU is likely to be different as compared to neonatal ICU (NICU). There may be a greater proportion of inborn babies in NICUs, as also will have significant numbers of preterm babies. On the other hand, neonates admitted to PICU are usually outborn babies with probably more severe illnesses. The measurement of severity of illness using scoring systems is gaining importance in intensive care. These scoring systems help in predicting mortality and morbidity and thereby can guide us in optimizing the limited health-care resources available in our country. They also help in improving the validity of outcome comparisons amongst different hospitals and units. These scoring systems assess the severity of illness in terms of degree of derangement from normal physiology across a number of physical and routine laboratory observations within a given time frame and are independent of diagnosis. Various scoring systems, e.g., the Score for Neonatal Acute Physiology (SNAP)(1), the SNAP perinatal extension (SNAP-PE)(2) and the Clinical Risk Index for Babies (CRIB)(3) have been used to assess the severity of illness among newborns. Of these, one of the most comprehensive scoring systems is the SNAP in which both the presence and severity of various physiologic abnormalities are scored. The SNAP score has usually been tested for applicability in a single neonatal ICU program with homogenous practice style. It has been primarily used in NICUs where newborns are admitted soon after delivery. In many centers, there is a common intensive care unit taking care of children and neonates. We analyzed the profile of newborns admitted to our hospital’s PICU over a period of 3 years and tested the applicability of SNAP scoring system in the neonates admitted. Subjects and Methods Data was extracted from the case records of consecutive newborns admitted to our six-bedded PICU in a tertiary care hospital in northern India between 2000 and 2002. Neonates with one of the following were excluded from analysis for SNAP: (i) death within 24 hours of admission; (ii) babies with lethal congenital anomalies; and (iii) in-complete medical charts. Standard definitions were used to categorize the neonates according to gestational age, birth weight and illness. SNAP score was calculated by adding up the scores for the 26 items(1). Data for stool gauaic was available only in a few patients where necrotizing enterocolitis was suspected. Primary outcomes measured were death in the PICU and length of stay in hospital. Statistical analysis was done using inter-cooled STATA 7.0 (Stata Corp., Houston, Texas). Receiver operating characteristic (ROC) curves were used to derive the best cut off value for SNAP. Appropriate tests for statistical significance were applied and P value <0.05 was considered significant. Results During the period of 3 years, 102 neonates were admitted to the PICU, constituting 14% (102/729) of total PICU admissions. Of these 5 neonates were excluded based on exclusion criteria. Out of the remaining 97 neonates, 70 (72.2%) were males. The mean age of babies was 12.92 ± 9.9 days (range 6 hours-28 days). Thirteen (13.4%) babies were born in our hospital and then readmitted and 84 (86.6%) were outborn. Fifty (51%) neonates were admitted with a diagnosis of sepsis, 11 (11.2%) had birth asphyxia and 9 (9.2%) had pneumonia (Table I). The mean duration of illness prior to hospitalization was 6 ± 6.6 days (range 4 hours- 12 days). Table I
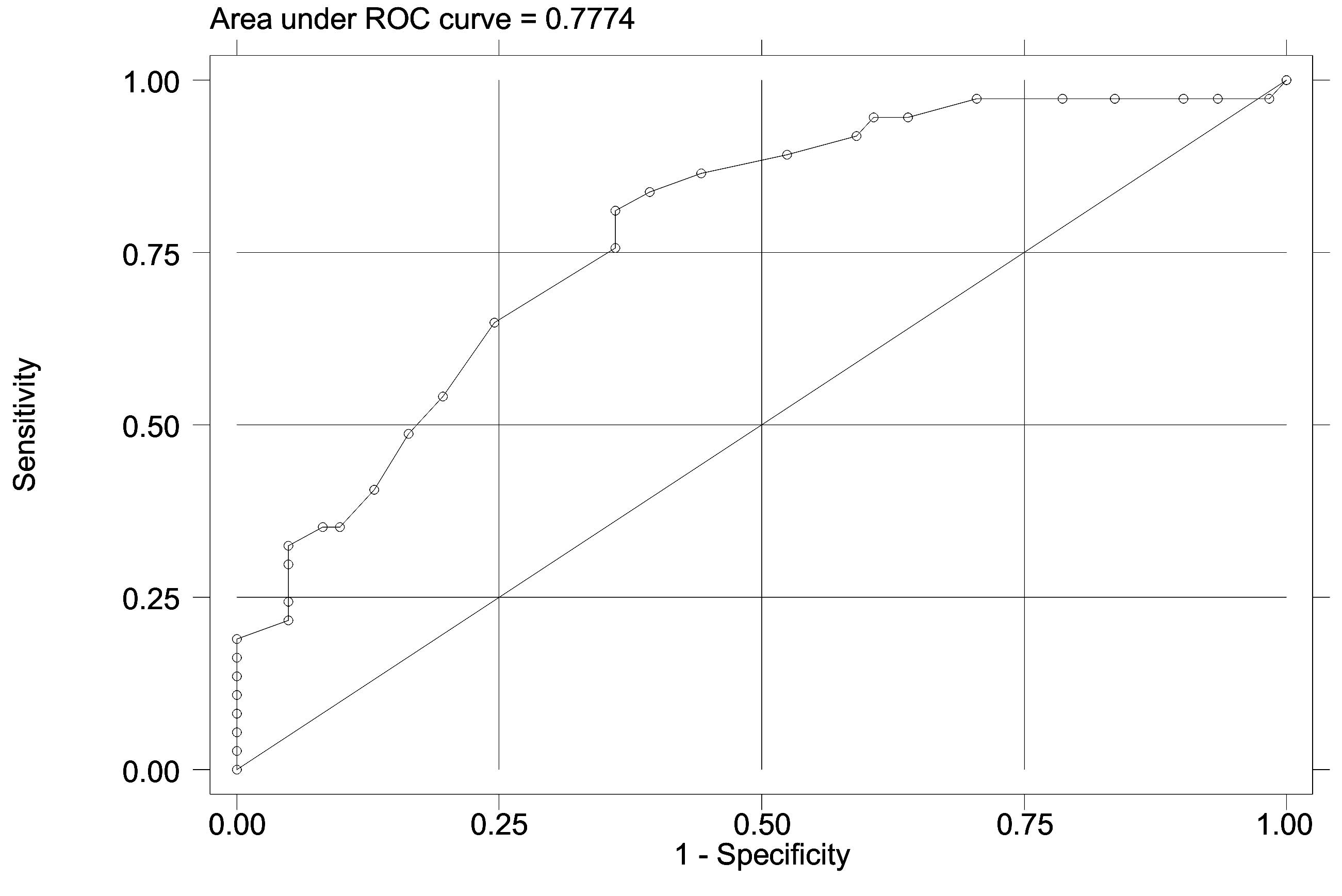
Thirty-seven (38.1%) of the neonates died in PICU while rest 60 (61.2%) were discharged. The SNAP score discriminated well between survivors and non-survivors; the area under the ROC curve for SNAP score was 0.777 (95% confidence interval 0.68-0.87) (Fig.1). The mean SNAP score in babies who died was 18.8 + 9.8 and 10.1 + 6.4 in survivors (P <0.001). Table II shows the mortality rates at different SNAP score cut-offs. The sensitivity and specificity of SNAP score equal to or greater than 15 in predicting mortality were 64.8% and 75.4% respectively. The positive and negative likelihood ratios at this cut-off were 2.63 and 0.47 respectively (Table II).
Table II Sensitivity, Specificity, Positive (LR+) and Negative (LR-) Likelihood Ratios at Various Cut off Points for SNAP Score.
The mean duration of PICU stay was 4.51 ± 7.8 days (Range 1-60 days) and mean length of stay in hospital was 15.2 ± 12.3 days (1-68 days). We did not observe any association between SNAP and length of stay (LOS) in hospital on multivariate analysis (P = 0.5). Sixty-two neonates were mechanically ventilated for a mean duration of 4.9 ± 5.76 days (range: 6 hours-24 days). Of these, 34 (54.8%) died. The mean SNAP in those who were ventilated was 14.5 ± 7.9. In this subgroup, the mean SNAP in those who survived was 10.53 ± 5.5 and in those who expired was 17.7 ± 8.09 (P = 0.003). Discussion In our PICU, 14% of all admissions over a 3 year period were neonates. The majority of these were outborn babies, admitted through the emergency services. In the absence of an extramural nursery in the hospital, our PICU usually provides care to such patients. Infections were the major reason for admission. This is different from the results of Maiya, et al., where hypoxic ischemic encephalopathy and hyaline membrane disease were the commonest admitting diagnoses(4). The development of severity of illness - measures is essential for the comparison of outcomes, health planning and clinical audit. It also helps in analyzing the costs of neonatal intensive care. SNAP was designed primarily as a measure of severity of illness and can separate infants into groups with 2 to 20 fold differences in mortality. It is valuable in making stratification possible in epidemiologic studies and in randomized controlled trials(5). We found that SNAP was a good predictor of mortality. Higher scores predicted higher mortality (Table II). Our results are comparable to previously reported studies(4,6-8). Multivariate analysis showed that higher SNAP score was associated with a higher mortality rate. SNAP also reasonably predicted mortality in ventilated babies. We did not observe any correlation between SNAP and LOS. Some earlier studies also reported similar findings(4,7). This could be explained by the fact that various clinical factors that are not included in the SNAP score like gestational age, birth weight and type of illness may influence the length of stay in hospital(9). Many of these factors are not represented in the scoring system. SNAP may be cumbersome because of the large number and complexity of items and also as it takes a long time to complete scoring. It also does not include diagnostic classification. Collection of data in the 24 hours after admission tends to blur the initial severity of illness with the success of therapy. The problem with such 24-hour scores is that they are affected by the treatment given after admission to the ICU. Neonates admitted to a unit with good quality of care will have lower scores than similar neonates admitted to a unit with poorer care who are not appropriately managed in the first 24 hours and the latter unit’s high mortality rate will be inappropriately attributed to its having sicker neonates. For assigning scores to various items in the SNAP score, the worst values in the first 24 hours are recorded. Therefore, SNAP cannot predict death of infants who die during the scoring period of 24 hours. In conclusion, neonatal sepsis and birth asphyxia were the most common indications for admission of neonates in our PICU. We observed that SNAP is a valid measure of severity of illness at admission in newborns. It helps in predicting the probable outcome in neonates admitted to the PICU. In most other studies, the score had been validated for newborns admitted early after birth. In our experience, the same score has performed quite well in neonates of different age. It can also help in improving the referral system, where babies with high scores can be referred for tertiary care at the earliest. In order to make it easy to use, it is desirable to simplify the SNAP or have another scoring system that uses patient data at admission. Contributors: AV participated in data collection and writing of manuscript. AM participated in data collection. RL participated in data collection, analysis and writing of manuscript and will act as the guarantor. SKK participated in analysis and writing of manuscript. Funding: None. Competing interests: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
![]()