|
|
Short Communication Indian Pediatrics 2007; 44:683-686 |
||||||||||||||||||||||||||||||||||||
|
Validation of the PELOD Score for Multiple Organ Dysfunction in Children |
||||||||||||||||||||||||||||||||||||
|
Anu Thukral, Utkarsh Kohli, Rakesh Lodha, S.K. Kabra and N.K. Arora From the Department of Pediatrics, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110 029, India. Correspondence to: Rakesh Lodha, Assistant
Professor, Department of Pediatrics, AIIMS, Ansari Nagar, New Delhi
110 029, Manuscript received: September 26, 2006; Initial
review completed: December 29, 2006;
It has been a consistent observation that intensive care unit mortality correlates with the number of failing organ systems and the degree of dysfunction within any given organ system. The reported frequency of multiple organ dysfunction in pediatric intensive care units is 11-27%(1-4). There is need to have objective measure of multiple organ dysfunction. In children, Pediatric Logistic Organ Dysfunction (PELOD) score was developed in prospective multicenter study by Leteurtre, et al. and validated by the same group in a multidisciplinary tertiary care pediatric intensive care unit of university affiliated hospitals(6,7). We conducted a study in a Pediatric ICU to identify the frequency of children who have multiple organ dysfunction at admission using the PELOD score, and its impact on the mortality. Subjects and Methods We prospectively included all consecutively admitted patients to the pediatric intensive care unit of a tertiary care hospital in north India over a 13-month period. The unit admits approximately 200 children annually. Data were collected in a predesigned collection sheet and included the demographic characteristics, reason for intensive care unit admission, and intensive care outcome. The data on the variables of PELOD score were recorded on day one. Variables were only measured if clinical status of patients justified their knowledge and it was assumed to be within the normal range if not measured. The most abnormal values were retained for the statistical analysis. All physiologic data accumulated during the preterminal period in dying patients (the last 2 hrs of life) were not considered for analysis(7). To calculate the PELOD score, each organ dysfunction received points for the single variable associated with the most points. The maximum number of points for an organ is 20, and the maximum possible PELOD score is 71(7). Organ dysfunction was identified if the score for any organ system was more than 0. Results During the study period, 209 patients were admitted. The male to female ratio was 1.78. Infants accounted for 41.2% of all admissions. In 37.2%, primary indication of admission was severe sepsis/ septic shock; respiratory distress requiring ventilation accounted the second largest category (25.6%); 13.5% admissions were due to a neurological illness, 11.7% had renal failure requiring peritoneal dialysis, and 3.7% of patients had more than one illness at the time of admission. Gastrointestinal, cardiac diseases, metabolic and the miscellaneous category constituted 2% each.
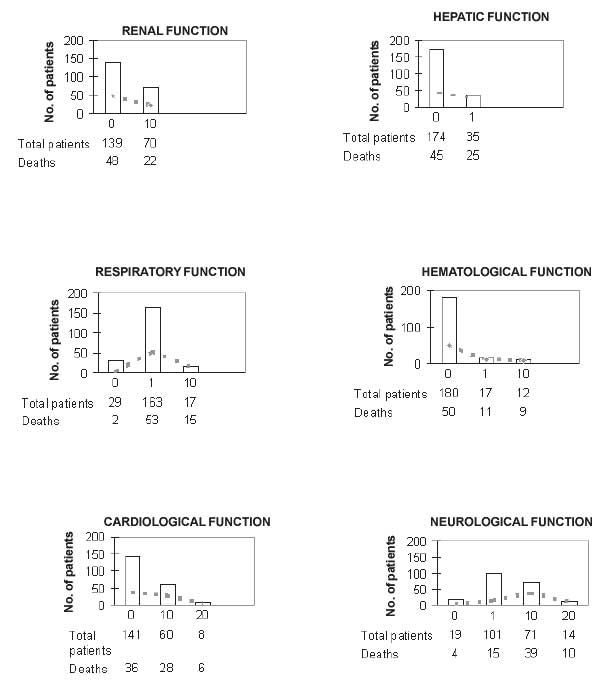
Ninety one percent of children admitted had multiple organ dysfunction. Three (1.5%) patients had no organ dysfunction, 16 (7.6%) had one, 76 (36.3%) had 2 organ dysfunction, 114 (54.6%) had 3 or more organ dysfunctions. Figure 1 shows the distribution of patients for each organ dysfunction and outcome. The area under the curve for predicting death using the PELOD score equation was 0.80. TABLE I Relation Between The Number of Organ Dysfunctions, Pelod Score and Mortality
Discussion The most common cause of ICU morbidity and mortality is the development of progressive physiological dysfunction remote from the site of primary disease, a phenomenon now termed as multiple organ dysfunction syndrome. The high frequency of organ dysfunction seen in our study indicates that children with greater severity of illness were admitted to the ICU. Because of the limited number of beds in our ICU, only the sickest children may have been admitted to the ICU. In addition, the referral nature of our hospital may lead to selection of more critically ill children. In other studies, it has been found that about 25% of the children admitted to PICU had MODS(3,4). The diagnosis of multiple organ dysfunction is supported by the observation in a critically ill patient of the simultaneous dysfunction of at least two organ systems. In children, the number of dysfunctional organs is frequently used to describe the severity of cases of pediatric MODS. This ordinal scale has been named the pediatric MODS score by some physicians. Two consecutive prospective studies were completed to develop and to validate the PELOD score(6,7). The development study of the PELOD score included 594 consecutive patients and 51 deaths. The discrimination of the PELOD score was 0.98 ± 0.01 (area under the receiver operating characteristics curve + SE). The calibration was good (p 0.44, 3 degree of freedom). A validation study was undertaken including total of 1,806 consecutive patients. The discrimination of the PELOD score was 0.91 ± 0.01 (area under the receiver operating characteristics curve + SE). The calibration was good (p 0.54, 5 degree of freedom). The relation between mortality rate and PELOD score in our study is good. The mortality rate with at least 2 organ dysfunction was 15.7% in our study; increasing from 6.3% for one organ dysfunction to 100% for six. Marshall and colleagues(5) reported that 57% of adult patients had no organ dysfunction, 25% had one and 18% had two or more and the mortality rate with at least two-organ dysfunction was 42% in Marshall’s study. PELOD score can detect organ dysfunction even in patients with a low mortality rate. The discriminatory capacity of PELOD score was good (the area under the curve being 0.80 in our study). The mortality was directly proportional to the degree of organ dysfunction and the PELOD score also increased with number of organ dysfunction. Children seem to develop MODS in a simultaneous way (not in the sequential manner) and much earlier(10). Furthermore, a consistent characteristic in the pediatric studies has been different patterns of organ involvement as compared with what occurs in adults(11). We found some differences with the findings reported in developed countries. The subjects under study were different. The majority of our patients, in contrast to those considered in other pediatric studies, had a medical condition rather than a surgical one. The age of our children was somewhat younger, and their stay was slightly longer. It is probable that there are important differences in socioeconomic levels between patients in PICUs of developed and developing countries. The PELOD score may be more clinically meaningful than PRISM-APS (Pediatric Risk of Mortality- Acute Physiology Score). The latter includes parameters related to different organ dysfunctions but does not allow separation of each organ dysfunction(12,13). Our study has a few limitations, one we include a few number of patients and two only intensive care unit mortality was considered (the latter was not a significant limitation since the previous studies had also compared the mortality at the end of intensive care unit stay and post intensive care unit mortality may be a significant problem in adults which is not the case in children). Another limitation could have been a treatment bias. PELOD score includes data that can be modulated by the care provided during PICU and hence cannot differentiate between therapy and severity of the disease. Contributors: RL, NKA designed the study. RL, SKK did analysis and were involved in manuscript writing. AT was involved in data collection, analysis, and manuscript writing. UK assisted in manuscript writing. RL would act as guarantor of the paper. Funding: None. Competing interests: None.
| ||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||
|
|
![]()