|
|
Case Reports Indian Pediatrics 2005; 42:942-945 |
||
|
Ocular Manifestations of Behcet’s Disease |
||
|
From the Department of Child Health and *Department of Dermatology, Christian Medical College, Vellore, 632 004, India. Correspondence to: Dr. Prabhakar D. Moses, Professor & Head, Department of Child Health, Christian Medical College, Vellore, 632 004, India. E-mail: [email protected]
Behcet’s disease is a systemic inflammatory vascular disorder characterized by recurrent oral and genital ulcers, uveitis arthritis and skin lesions. It has a world- wide distribution with clustering among populations having a high prevalence of HLA-B5. There are only a few reports of Behcet’s disease with ocular manifestation in children from India. Case Report An 8-year-old student from West Bengal presented with a history of fever, recurrent oral and genital ulcerations, skin pustules and joint swelling for 4 months. There was a history of bilateral parotid swelling at the onset of illness. He had been hospitalized elsewhere for 2 months for the above symptoms and had received antibiotics, IV Immunoglobulin, two blood transfusions, and was on nasogastric feeds.
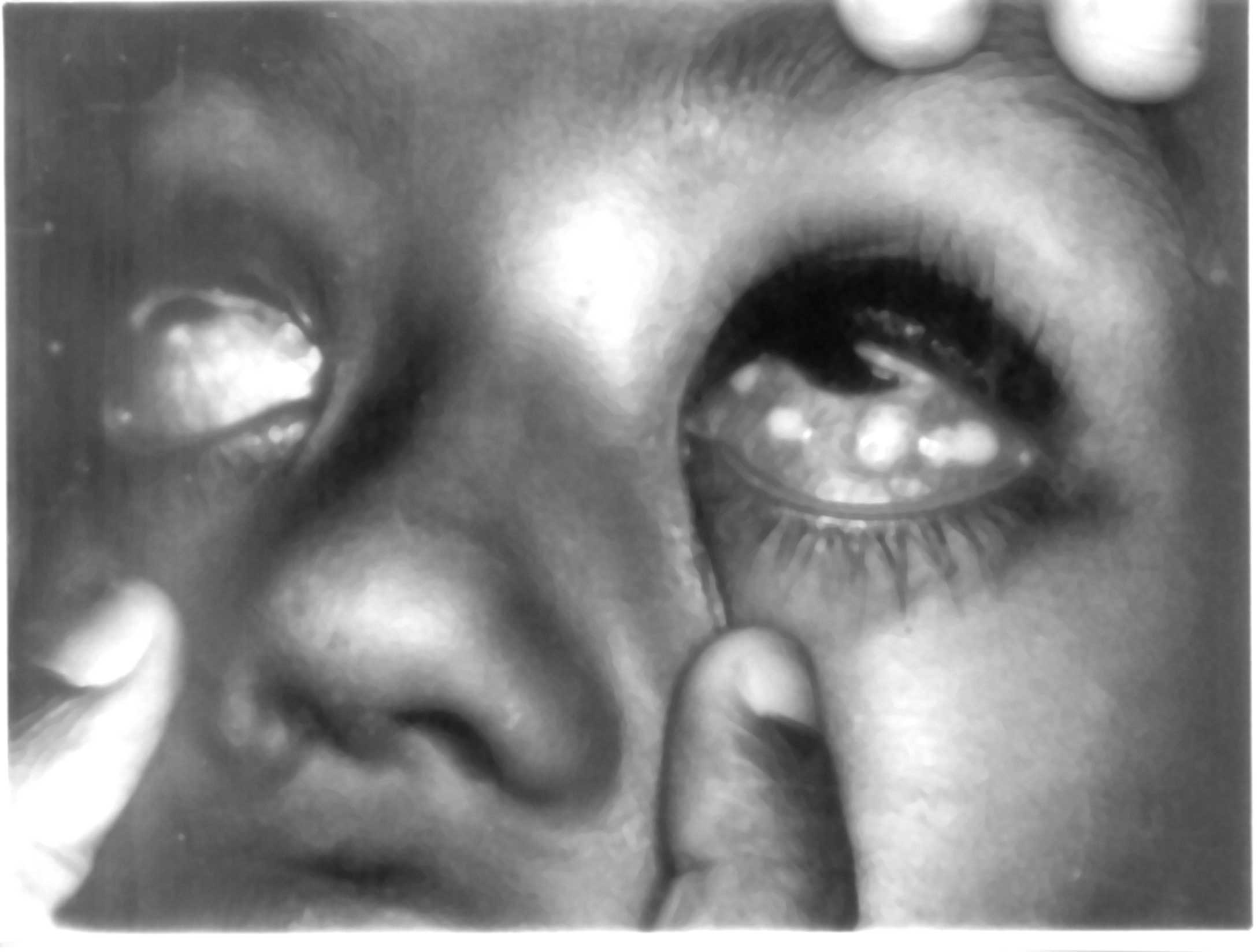
On examination child was febrile (102ºF) toxic and undernourished. Weight was 17.7 kg. He had bilateral enlarged tender submandibular and upper deep cervical lymphnodes. Ocular examination revealed nodules over the bulbar conjunctivae, conjunctival congestion and bilateral purulent eye discharge (Fig.1). Fundus examination was normal. He had multiple oral ulcers, few covered with slough and few covered with crusts, seen on the tongue and upper and lower lips. There was a pustule on the left angle of mouth. Multiple pustular lesions of size 1-2 cm were present over the face, arms, both knees, dorsum of the feet and IV puncture sites; some had healed and left scars. Perianal and periurethral areas were normal. Tender swelling of right knee joint with minimal effusion was present. The examination of other systems was unremarkable. Hemoglobin was 10.6 g/dL. Total white cell count was 21,400/mm3 with 90% neutrophils. Platelets count was 5,89,000/mm3. Liver function test, S. creatinine, urea, calcium and electrolytes were normal. ANA, Rheumatoid factor and LE cell preparation were negative. Serum complement was 80%. VDRL was non-reactive; CRP was positive 94.6mg/L. HIV serology and HBs Ag were negative. Smear & culture from the buccal ulcer was negative for Herpes simplex virus. Pus swab culture from ulcer in the right foot grew Pseudomonas aeruginosa. CSF analysis was normal. HLA typing was positive for B52(5). Chest X-ray was normal. Ultrasonography of abdomen and upper gastrointestinal endoscopy were normal. Slit lamp examination of his eyes revealed no evidence of uveitis. Bone marrow smear showed hypercellular marrow with mild increase in reactivity and biopsy showed hypocellular marrow with myeloid hyperplasia. Skin biopsy from right leg showed intra-epithelial vesicle with neutrophilic infiltration, deep dermal granulomatous inflammation, moderate perivascular chronic inflammation and telangiectasia in the dermis. Pathergy test was positive. At admission the differential diagnoses considered were connective tissue disorder, immunodeficiency syndrome, lympho-proli-ferative disorder, and disseminated HSV infection. He was initially treated with IV antibiotics and intravenous acyclovir. Later the possibility of Behcet’s disease was considered in view of the oral ulceration, typical skin (vesicles, pustules and pyoderma gangrenosum) and eye lesions, genital ulceration and positive pathergy skin test fulfilling the recommended diagnostic criteria(1). HLA typing was positive for HLA B5 and skin biopsy was suggestive of Behcet’s disease. He was started on oral prednisolone (60 mg/m2/day) and local eye application of Fluromethonolone drops. He became afebrile from the 2nd day of starting steroids; skin and ocular lesions also improved. Right knee joint swelling was treated with skin traction and it resolved within one week. He was discharged on oral feeds. At follow-up a month later his skin lesions had improved and the steroid dose was tapered and stopped after 4 months. Two weeks later he presented with recurrence of eye lesions and oral ulcerations. He was restarted on oral steroids and continued for a year and stopped . At his last visit one and half years after the diagnosis and one month after stopping steroids, he was well with no skin or oral lesions. The parents were counselled regarding the prognosis and the risk of recurrence of manifestations of the disease. Discussion Behcet’s disease was first described by Hippocrates in ancient Greece and later by Behcet, a Turkish dermatologist. An international study group had proposed a set of criteria to diagnose Behcet’s disease(1). These are recurrent oral ulcers plus any two of four other manifestations (a) recurrent genital ulcers, (b) eye lesions, (c) skin lesions and (d) positive pathergy test. The etiology of Behcet’s disease is unknown. Data suggests that genetic and other environmental factors of viral and toxic origin may contribute. Virus like particles were shown in tissue taken from the glomerular basal lamina, iris, choroid and retina. Exposure to organic phosphates, organo-chloride pesticides, and polychlori-nated biphenyls may cause clinical symptoms similar to those of Behcet disease(2). Behcets disease in children is regarded as uncommon and most information limited to case reports(3). The eye inflammation, which is one of the most important organ involvement of the syndrome, is encountered in half of the patients. It may manifest as uveitis or conjunctivitis. Eye disease is more commonly seen in males and younger patients and the prognosis is poor(3). HLA-B 5 antigen is characteristic of patients with eye disorder which occur in 84% of Turkish patients(2). Panda, et al.(4) reported the clinical profile of 58 patients with Behcet’s disease in India, which included 5 children under the age of 12 years. The children in his series had less ocular manifestation(4). In contrast our child had ocular manifestation. Amman, et al.(5) in his series of 6 children with Behcet’s disease reported one child with ocular involvement (keratocon junctivitis)(5). Konepaut in his international collaborative study of children with Behcet’s disease reported eye lesions in 61% (40 of 65). Conjunctivitis was seen in 4 of the 65(3). The primary clinical manifestation of Behcet’s disease is oral ulceration. It is the initial symptom in greater than 60% of patients and is ultimately present in more than 90%(5). However, it is known that 1-3% of patients manifest other signs of the disease but not oral ulcerations. Genital lesions appear as small red elevated acne-like lesions and evolve to slow healing punched-out-like lesions. They mostly heal with a residual scar. Compared to the oral lesions, genital ulcers are fewer in number, and it takes a longer time for them to heal. The skin manifestations of Behcet’s syndrome can be grouped into three: (i) nodular red, painful swellings; (ii) acne-like lesions; (iii) lesions associated with diseases of skin vessels. Pathergy reaction is the production of a blister or a pustule in response to puncturing the forearm skin with a sterile needle. The reaction, which appears within 24 hours and maximizes in 48 hours, is a 1-2mm elevated lesion surrounded by a reddish area. Joint involvement is one of the major complaints of the patients. The commonly involved joints are the knees, ankles, wrists and elbows in decreasing order. Joint destruction is not seen and it is self-limiting lasting 1-2 weeks. Acknowledgement We like to acknowledge the contribution of Dr. Rekha Solomon, Lecturer, Child Health Department towards the care of the child and preparation of the manuscript. Contributors: SEA was involved in drafting the paper. PDM critically reviewed the manuscript. He would act as the guarantor for the paper. RG assisted in confirming the diagnosis and managing the patient. Funding: None. Competing interests: None.
| ||
|
References | ||
|
![]()