Shanthi Ananthakrishnan
and P. Nalini
From Jawaharlal
Institute of Post Graduate Medical Education and Research (JIPMER),
Pondicherry, India.
Correspondence to: Dr.
Shanthi Ananthakrishnan, Type 5/1, Danvantri Nagar, Pondicherry 605
006, India. E-mail:
[email protected]
Manuscript received:
November 28, 2001, Initial review completed: December 26, 2001;
Revision accepted: March
6, 2002.
This study was
conducted to estimate the magnitude of school absenteeism and
determine its causes in a village in Tamilnadu. The sample included a
cohort (n=143) followed for one year and a cross sectional sample (n =
278). The mean number of episodes of school absenteeism was 1.6 ±
0.6/ child/year and the mean number of days lost was 1.5 ± 1.4
days/child/year. It is estimated that on a working day of the school,
about 0.85% of the student population will be absent. Common causes of
absenteeism were adverse weather conditions, work, illness and social
customs. School absenteeism was found to be higher during rainy season
and local groundnut picking season (October-December) than during
other months. If possible, school based programs may be avoided during
months with maximal absenteeism.
Key Words:
School absenteeism, school based programs.
Schools are increasingly
being recognized as effective tools to reach the community(1). School
based screening and intervention programs have helped in developing and
implementing control measures for several disorders of public health
importance(2-4). However, the effectiveness of these programs depends on
the number of children attending schools. School absenteeism is an
important issue, which affects not only educational achievement but also
results in false estimation of the prevalence of disease in school based
screening programs. Further, school based intervention programs may miss
out several affected children(5,6). This study was, therefore, carried
out to estimate the magnitude of school absenteeism and identify its
causes.
Subjects and Methods
The study was carried out
in Kedar (population, 3,000), a village in Tamil Nadu, about 65 km. to
the southwest of Pondicherry, South India. Basic demographic details of
the village was obtained by doing a house to house survey. The
objectives of the study were explained to and informed consent was
obtained from the village leader, parents, teachers and children to
participate in the study. Most of the villagers were either landless
agricultural labourers or weavers and were socioeconomically backward
with an average per-capita income of Rs. 2,201 ± 36 per annum. The
village has 2 government schools - a primary school and a high school
with a middle school section. A total of 1,881 children were studying in
the school out of which about 50% were from neighbouring villages. There
is a government sponsored midday meal scheme providing supplementary
nutrition (300 - 400 calories and 15- 20 g protein per day/child) to all
children studying in both the schools.
Out of a total of 658 families in the
study village, 100 families were randomly selected and all children
studying in school from these families formed the cohort. They were
followed up fortnightly for one year. Information on school attendance
and reasons for absenteeism, if any, was obtained and entered on a
structured format.
In a cross sectional
survey, classes I-X of the government schools in the study village were
visited at the rate of one class per day on 10 consecutive working days
in the mornings. In each class, students who were absent the previous
day, but were present on the day of the visit were interviewed with a
structured questionnaire as to the cause of absence the previous day.
Data were obtained only from those students who had absented themselves
the whole day.
Statistical tests used
for analysis were chi-square test for comparing proportions and Student’s
‘t’ test for comparing means. Alpha error was fixed at 5%.
Results
Cohort Study
There were a total of 664
children attending school from the study village out of which 143
children including 54 girls and 89 boys were in the cohort. In the study
village, the proportion of children between 5-17 years of age who had
been enrolled in school at sometime or the other was 89.5%. However, at
the time of study, the proportion of children actually attending school
in the primary section (5-11 years), middle school section (12-14 years)
and high school section (15-17 years) were 80.8%, 80.5% and 53.4%
respectively.
Over a period of one
year, 30 out of 54 (55.5%) girls and 40 out of 89 (44.9%) boys had
absented from school on one or more occasions. The total number of days
lost was 210 and the mean number of days lost was 1.5 ± 1.4
days/child/year (estimated for the cohort; n = 143). The total
number of episodes of absenteeism was 110 (50 in girls and 60 in boys).
The mean number of episodes of school absenteeism was
1.6 ± 0.6/child per year (estimated for those who
were absent; n = 70). There was no significant gender difference
in either the number of episodes of absenteeism or the number of days
lost (P > 0.05). Given the total number of working days in an
academic year as 180 and a mean loss of 1.5 days/child/year, in the
study school which has a strength of 1,881 students it is estimated that
on any working day about 16 students (0.85%) are likely to be absent.
Out of all absenteeism episodes, 53.6% were among primary school
children, 33.6% among middle school children and 12.7% among high school
children. The maximum number of episodes (66.3%) of absenteeism occurred
during the monsoon months, (October-December) and the minimum (9.1%)
between January-March.
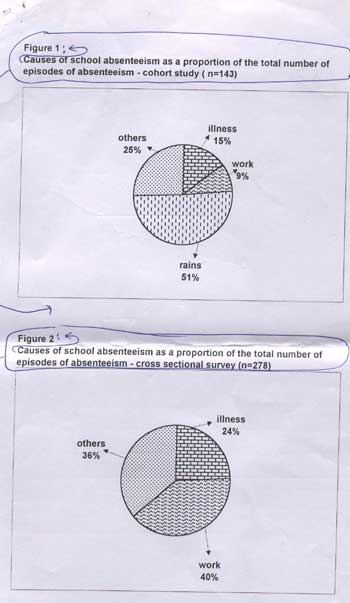
The most common cause of absenteeism was
inclement weather conditions during monsoon followed by other causes
such as social functions at home/village and social visits (Fig. 1).
Illness or work was not a major cause of school absenteeism. One episode
of
absenteeism was due to an
acute illness in the mother. The mean number of episodes of school
absenteeism due to illness was 0.22/child/year and the mean number of
days lost due to illness 3.2 ± 2.2 days/episodes and the corresponding
figures for work were 0.12/child/year and 1 ± 0.5 days/episode.
Cross Sectional Survey
A total of 278 children
(117 girls & 161 boys) were found to be absent during the cross
sectional survey. Highest number of absentees were in the middle school
section (59.3%) followed by primary school (24.8%) and high school
SECTIONS (15.8%). The most common cause of absence was work followed by
illness and other causes (Fig.2). The survey was conducted in
October which happened to be groundnut picking season in that area. Many
children had gone to pick groundnuts and hence work (extra scholastic)
was observed to be the most common cause of school absenteeism. Apart
from groundnut picking, the nature of work that caused school absence
was often trivial such as fetching water, carrying food, going to the
market etc. which took about one hour only. Illness (24.1%) as a
cause of absenteeism was significantly less (P < 0.05) than that due
to work (39.6%) or other causes. Illnesses that caused school
absenteeism were fever, headache and abdominal pain. There was no
significant gender difference with respect to the cause of absenteeism
(P > 0.05).
Discussion
The current study shows that school
absenteeism is not a major issue among school children in the study
village. This is perhaps due to the mid-day meal scheme which has been
effective in improving school enrollment and attendance(7). The higher
proportion of work as a cause of school absenteeism in the cross
sectional survey could be due to the fact that the survey was conducted
during groundnut picking season when many children especially in the age
group 10-15 years were away for picking groundnuts. In areas where there
are seasonal crops and school children are useful in field work, school
timings could be made flexible so that children could learn and earn at
the same time. The reality in the village is that there is tremendous
economic pressure from the family for the child to earn and add to the
family income whenever possible. In this context, flexible school
timings will atleast ensure that the child gets some education since,
children preferred to stay away from school rather than attend late
since it involved punishment or fine. Rigidity in the educational system
in the presence of economic pressure might drive the child away from
learning to earning and eventually lead to dropping out of school.
Adverse weather
conditions during monsoon was to a large extent responsible for school
absenteeism in this study. The main reasons for this could be that most
of the classes functioned from thatched sheds which could not brave the
rains besides inability of some children (particularly those who are
from neighbouring villages) to reach the school due to difficulties in
commuting. School based screening and intervention programs could
therefore be avoided during these months in the study village.
A common cause of school
absenteeism observed in the present study was social functions at home
and in the community. Children were often asked to stay at home to help
or to escort female members of the family to neighbouring villages to
attend some functions. This points to a lack of discipline among not
only children but also elders and the priortization of social customs
over education.
Since this study
pertained to only a particular village, the conclusions cannot be
generalized. Further studies need to be carried out in several areas
varying in literacy rates, social and cultural values, etc.
before drawing meaningful and relevant conclusions on school
absenteeism.
Contributors:
SA designed and conducted the study and shall act as guarantor for the
paper. PN helped in designing the study. The manuscript was written by
both the authors.
Funding: None.
Competing interests:
None stated.
|
Key
Messages |
| •
School absenteeism in general and due to illness in particular are
not important problems among school going children in rural Tamil
Nadu. |
