|
|
Original Article Indian Pediatrics 2002; 39:819-825 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Urinary Citrate Excretion in Idiopathic Nephrolithiasis |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Simmi K. Ratan, V. Bhatnagar, D.K. Mitra, N. Basu, L.K. Malhotra
CITRATE, a by product of normal oxidative pathways in the body, is normally excreted in the urine. Tubular absorption of citrate varies with the mitochondrial pH gradient. Thus, a delicate balance is maintained at physiological range of pH of body fluids, with alkalosis increasing and acidosis decreasing the urinary citrate output. Most therapeutic agents causing alteration of citrate excretion usually work through the final pathway of altering pH of the tubular fluid(1-2). Besides, the citrate output in urine can also decrease as a result of gastrointestinal disturbances leading to a decrease in citrate absorption(3-4). Citrate is an important inhibitor of urolithiasis, which forms soluble complexes with calcium and inhibits precipitation of calcium oxalate and phosphate, and growth of their crystals(2,3,5-8). Several previous studies have evaluated urinary citrate levels in patients with urolithiasis and in normal individuals. The results have been conflicting; some have shown low urinary citrate output in stone formers as compared to controls(5,9,10), while other studies have shown no difference (8,11,12). Even the range of 24 hours urinary citrate excretion in normal subject has been wide(1). Differences in the method for citrate estimation or the variations in the composition of diet may be responsible for this phenomenon(3). Most of the previous studies have been on adults, children forming a small fraction in some of these studies(13,14). In an elegant study, Miyako, et al. have found that urine from children, by virtue of high concentration of inhibitors, as compared to adults, disfavours stone formation(15). They, however, did not compare the urinary inhibitor excretion in normal and stone forming children. We have studied urinary citrate levels in stone forming children and age/weight matched controls. To the best of our knowledge, such a study has not been reported in children. Subjects and Methods Fifty children, up to 12 years of age, admitted for removal of either bladder or kidney stones, over a period of 5 years, from January 1989 to December 1993 were studied. Three children with metabolic diseases or known predisposing factors for stone formation were excluded. A total of 150 children admitted with problems other than those pertaining to the genitourinary system (and no evidence of urinary tract infection), formed the control group. The controls and study patients were from north-west India, belonged to similar socio-economic status and were matched for age and weight. In those with urinary tract infection, citrate estimation was deferred till there was microscopic and culture proven evidence of clearance of infection. No dietary restrictions were imposed and the subjects were advised to maintain an optimum fluid intake throughout the study period. The subjects were not on any drug e.g., acetazolamide and thiazides, that could have altered the blood or urinary levels of citrate or calcium. Imaging and functional studies included x-ray of the abdomen, ultrasonography, intravenous pyelography and/or diuretic renography to assess anatomic abnormalities, urinary obstruction and back pressure changes. Urine pH was measured and the 24-hour urine estimated for calcium, creatinine, sodium, potassium and uric acid. Blood levels of pH, bicarbonate, calcium, phosphate, uric acid, creatinine, urea, sodium and potassium were measured. For estimation of citrate, the 24-hour urine was collected in a container using 10 ml of 10 N sulphuric acid as preservative. Citric acid estimation was done using the colorimetric method based on oxidation of citric acid in urine to pentabromacetone and the absorbance read at 445 nm(16). This method was chosen for its sensitivity, feasibility and high reproducibility of results. Urinary citrate levels estimation were expressed as mg/g creatinine. Patients with citrate excretion below 2 standard deviations (SD) were diagnosed as hypocitraturia. For purposes of comparison, the children were divided into 3 groups: Group 1 (1-4 years), Group 2 (5-8 years) and Group 3 (9-12 years), for either sex. The distribution of the number of subject in each of these groups is shown in Table I. The stones removed were dried, powdered and examined by x-ray diffractometry (Giegerflex-D/ax-RB-RU 2000, Rigaku Corporation, Japan). The stones were identified by comparing the diffraction value with standard data. Due to technical reasons, only 35 stones were analyzed. Statistical Methods Mean values and SD was calculated for each of the three age groups. Chi-square test was applied to compute the significance of the categorical variables; p < 0.05 was considered marginally significant and p < 0.01 was considered significant. Table I-Weight distribution and citrate excretion (mean ± SD) among patients and controls
* Statistically significant lower excretion of citrate compared to controls ( P < 0.01) # No statistically significant difference between males and females in any age group for patients or controls
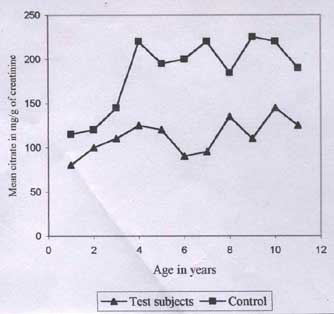
Results There was an overall preponderance of urinary stones in males; the highest incidence of urolithiasis was seen between 3 and 4 years of age (group 1) (Table I). We found all study patients to have a relatively higher excretion of calcium as compared to controls, although the difference was not statistically significant. Excretion of citrate in 24-hour urine sample was significantly lower in patients as compared to controls, for males in all Groups. Females in Group 3 also showed a significantly lower citrate excretion, though those in Groups 1 and 2 showed only a marginally lower citrate. There was no significant difference in the urinary citrate excretion between males and females in any Group. The urinary citrate excretion versus age showed similar pattern for patients and controls (an increase in citrate excretion with increasing age), but the levels in stone formers were lower (Fig. 1). Depending upon the constituents, four main type of stones were identified namely, calcium phosphate, calcium oxalate, uric acid and magnesium ammonium phosphate. Of 35, 9 stones had at least more than one major constituent. Table II shows the distribution of these stones and the mean level of urinary citrate in different stones. Two boys in the Group 3 and one girl in Group 2 showed statistically higher levels of urinary uric acid. These three patients had calcium oxalate stones. Since the serum uric acid was within normal limits and there were no features of disturbed purine metabolism, this finding was believed to be consistent with the observation that idiopathic calcium oxalate stone formers generally have a higher uric acid excretion. Hypocitraturia was detected in 43% cases. The incidence was 76% for calcium phosphate, 87% for calcium oxalate, 40% for uric acid stones and 50% for magnesium ammonium phosphate stones.
Fig. 1. Agewise distribution of mean urinary citrate levels (mg/g creatinine) in controls and study subjects Table II-Citrate Excretion (mean ± SD) in Major Stones (n = 35)
9 stones had more than one component Discussion The role of urinary inhibitors was considered on the basis of the observation that even under normal circumstances the urine is supersaturated with stone forming constituents, whereas stones do not always form so often(6). Several other potential stone inhibitors e.g., macromolecules (glycosamine glycans, heparin, acid mucopolysaccharides), pyrophosphates, metal ions (zinc, fluoride, tin), and dyes (methylene blue) have been identified in the urine. Their role has been studied in in vitro studies and their levels compared in stone formers with normal subjects(3,5-12,17-25). It has been further observed that the role of a particular inhibitor may vary its concentration, urinary pH, the relative availability of other constituents and even in different individuals (3,6,7,17,19). Above all, they may affect different stages of stone formation. Thus, while some inhibitors affect the process of nucleation, others inhibit the growth and aggregation of stone crystals(7,17). Citrate has been widely studied for its stone inhibiting action in urine and it has been found to be particularly effective against the calcium oxalate and phosphate stones(3,5-8). An incidence of hypocitraturia in 46% of stone formers is reported(13,14). Both these studies have been from Turkey, a country known to have a high incidence of urolithiasis. In our study, the subjects hailed from north-west India (a stone endemic area of the country) and we found a comparable incidence of hypocitraturia (43%). While in previous studies, children comprised only 25% of the study population(13,14), our study has focussed entirely on children. It is quite obvious from these studies, as well as from ours, that in absence of any predisposing causes like anatomic defects, infection or metabolic diseases, hypocitraturia is an important cause of stone disease in endemic areas. Schwille, et al reported a higher incidence of hypocitraturia among patients with calcium urolithiasis (50-70%) compared to those with uric acid lithiasis (12-20%)(5). In yet another study, they did not find the citrate excretion to differ among patients with different types of stones(3). In the present study there was no statistically significant difference in the mean citrate excretion in children with different stone compositions, in either sex. A wide range of values for the urinary levels of citrate have been obtained even for normal subjects(1,5,18). It is known that a number of variables affect citrate excretion. These include age (lower in infants than in adults), weight (increases with increase in weight), urinary pH (decreases in acidic pH), diet (increases after food intake, especially after a high sucrose diet), sex hormones (higher in females due to higher estrogen concentration), metabolic acidosis (decrease in the output) and urinary infections (decreased levels)(1-3,10). Many body tissues, including the kidney, are also known to metabolize citrate. A low citrate output in stone formers is speculated to be due to reduced renal function, increased bacterial or renal metabolism and alteration of tubular pH, especially in patients with renal tubular acidosis(1-3,10). Other studies have shown no difference in citrate output among stone formers and normal individuals(8,11,12). Some authors have pointed out that different methods of citrate analysis may be the cause of these conflicting results(5). The enzymatic method (citrate lyase enzyme) gives more accurate results than the colorimetric method, as there is a possibility of interference with other chromogens in the latter(10). In the present study the colorimetric method based on the estimation of pentabromacetone was used because this simple method is known to give good results with high reproducibility(16). Since citrate excretion increases with increase in body weight, urinary citrate excretion in relation to creatinine gives a better assessment of stone risk(18). Using this method, the normal values for urinary citrate excretion for the Indian male were found to be 385.1 ± 41.1 mg/g of creatinine. In the present study, the values for citrate among normal and stone forming children were computed based on age and sex. We found significantly lower urinary citrate excretion in stone formers in all Groups for males and for females in age group 9-12 years. Although a detailed work up to exclude rare conditions e.g., cystinuria, hyperoxaluria were not done, this study suggests that citrate deficiency is associated with urinary stones in children. Dietary supplementation of sodium and potassium citrate increases urinary citrate level and decrease stone formation in 97.8% patients with low citrate(21). The cause of low urinary citrate levels is not clear; dietary(12), associated low magnesium or potassium levels(3) patients defective resorption of citrate from intestines(22) or increased renal destruction(4) may contribute. Studies comparing serum and urine levels of citrate in stone formers and controls can pinpoint the causal mechanism and guide therapeutic strategies in individual cases. Contributors: VB and DKM designed the study, supervised the analysis and drafted the manuscript; VB will act as the guarantor for the paper. SKR monitored patients, collected and analyzed the data. NB performed urinary citrate estimation and LKM the stone analysis.
Funding: None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()