1. In lung conditions, where infants require
aggressive ventilation (e.g. severe meconium aspiration syndrome or
PPHN), it may appear that the VG method is not effective with
constant low tidal volume (VT) alarms. This is frequently due to a
reluctance to set the back-up pressure high enough to allow the
ventilator to reach target VT. In this case, the options are:
(a) Increase the back-up pressures high
enough to allow the target VT to be reached. This is based on the
premise that volutrauma – and not barotrauma – causes lung damage
[2]. Therefore if the volume is appropriate, the pressure needed to
achieve that volume is irrelevant.
(b) As some people remain unhappy using
high peak inspiratory pressures, the alternative is to switch to
high frequency oscillation.
(c) It is always important with any mode
of ventilation to check that the amount of ventilator support
required is in line with the clinical situation. If not, other
contributory causes of poor ventilation (e.g., blocked
endotracheal tube, pneumothorax) should be excluded .
2. Infants can actively tighten their abdominal
muscles that can prevent gas entering the lungs during inflation;
often termed ‘splinting’ [3]. Forced expiration and splinting cause
hypoxemic episodes due to low lung volume and low VT delivery,
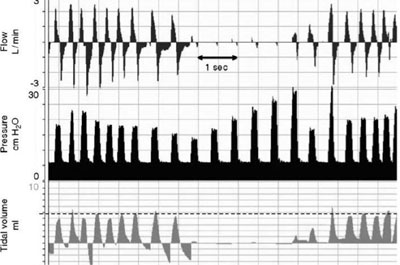
causing obstruction’ and ‘low VT’ alarms. Fig. 1 shows
a recording from a 1000-g baby ventilated with assist control (AC)
and VG ventilation at a rate of 50 per min, a set peak inflating
pressure (PIP) of 40 cm H2O, and a set VT 5 mL. It illustrates the
effect on the inflating pressure when the baby tightens the
abdominal muscles enough to temporarily stop inflation. This is
preceded by active expiration. During the first ten inflations, the
pressure is modulated to maintain the expired VT. During inflations
7, 8 and 9, the expired VT is larger than set VT and so the pressure
is reduced. At inflation 10, there is a very small VT, and therefore
the pressure is increased by 3 cm H2O for each
inflation for the next five untriggered inflations until a VT is
produced. This is then followed by triggered inflations at a similar
inflating pressure to the start of this recording, with one
untriggered inflation in between. A higher Pmax setting may allow
the ventilator to increase the PIP and overcome the obstruction more
quickly [4].
 |
|
Fig. 1 Ventilator recordings
showing effect of ‘splinting’ in a neonate on Assist Control
Volume Guarantee Ventilation.
|
1. Razak A. Guaranteeing the volume guarantee
ventilation. Indian Pediatr. 2015;52:444.
2. Keszler M. Volume-targeted ventilation. Neo
Reviews. 2006;7:e250-7.
3. te Pas AB, Wong C, Kamlin CO, Dawson JA, Morley
CJ, Davis PG. Breathing patterns in preterm and term infants immediately
after birth. Pediatr Res. 2009;65:352-6.
4. Klingenberg C, Wheeler KI, Davis PG, Morley CJ. A
practical guide to neonatal volume guarantee ventilation. J Perinatol.
2011;31:575-85.


