|
|
Research Papers Indian Pediatrics 2007; 44:751-759 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Clinico-epidemiological Profile and Validation of Symptoms and Signs of Severe Illness in Young Infants (<60 days) Reporting to a District Hospital |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
*** *Department of Pediatrics and @Department of Microbiology, Post Graduate Institute of Medical Education and Research, Chandigarh; **General Hospital, Sector 16, Chandigarh, #Murdoch Children’s Research Institute, Royal Children Hospital and University of Melbourne, Melbourne; ***WHO-HQs Geneva Office.
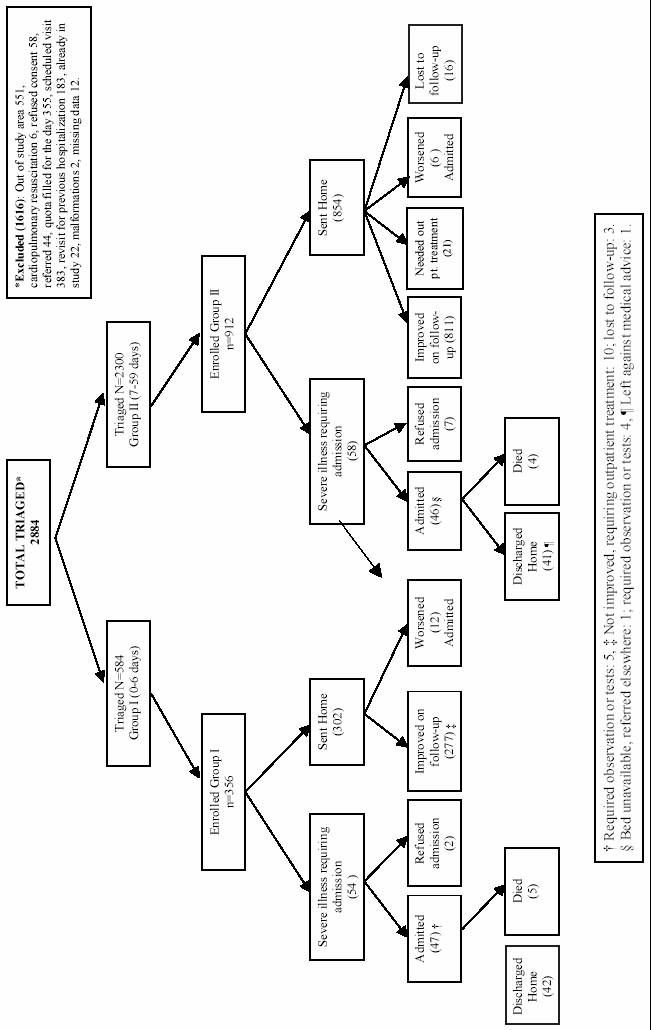
THE majority of babies in our country are delivered at home either by traditional birth attendants or family members. These newborns have their first contact with the health worker in the first weeks of life. The ANMs and other community health workers are trained with the help of IMCI (integrated management of childhood illnesses) guidelines which are designed to pick up babies with severe illness. However, these guidelines do not cover the assessment of newborns presenting in the first week of life(1,2). Hence, these have been adapted in India as the IMNCI (integrated management of neonatal and childhood illnesses) guidelines, by adding components of newborn care(3). However, these are consensus-based and have not been validated. Very scant scientific data are available on the potential value of different clinical features to identify the sick infant in the community. Therefore, the WHO initiated a seven country study designed to identify simple clinical symptoms and signs that would help health worker in developing countries to identify young infants less than 2 months of age suffering from serious illness. The objectives of the study were to describe the clinical and epidemiological profile of infants less than 2 months of age reporting to a district hospital and to assess the value of simple clinical symptoms and signs that can be used by health workers for detecting severe illness warranting hospital admission. This communication summarizes the results from the Chandigarh site in India. Methods This prospective study was conducted at General Hospital, Chandigarh in collaboration with Post Graduate Institute of Medical Education and Research (PGIMER), between May 2004 and May 2005. Chandigarh is a compact union territory of 114 sq km with a population of about 1 million and has few pockets of rural areas and urban slums. The General hospital is a 500-bed district hospital which caters to the population of union territory of Chandigarh, Mohali, Panchkula and adjacent rural areas. It runs a general pediatrics OPD (average attendance 200/day) and has a 50 bed pediatric ward. PGIMER is a tertiary care referral hospital with 1400 beds and is located less than one km from the General Hospital. It mainly caters to the referral population of many North Indian states. The detailed study methodology was similar to that of the other Indian site at Delhi which is being reported in this issue(4 ). However, there were minor site specific differences. The initial assessment at this site was done by an ANM (study person A) instead of a nurse at the Delhi site. Prior to actual start, a pilot study was conducted for 1 month (123 babies) in which orientation and training of personnel and testing of study procedures and forms was carried out and a manual of standard operating procedures was developed. The training of ANMs was done with the help of videos and actual demonstration of clinical signs on babies. The eligibility and exclusion criteria were the same as reported earlier(4). Eligible young infants presenting to the hospital between 8 AM and 8 PM on working days were screened by a triage person for inclusion and exclusion criteria. During the morning and afternoon shifts, babies were recruited from the OPD and emergency departments, respectively. Pulse oxygen saturation (SpO2) of all infants was measured using an Eagle 1000 pulse oximeter (Wipro GE, USA). Other monitoring, quality control, follow-up, data management and analysis was similar to the other site. Ethical clearance This study was approved by the Ethics Committee of PGIMER, the WHO Ethical Research Committee and the Indian Council of Medical Research. Results A total of 2884 infants under two months of age were screened in the OPD by the triage clerk. Of these, 1268 were enrolled into the study and examined by the ANM and pediatrician -. The reasons for exclusion of the remaining are shown in Fig. 1. The reasons for seeking care as conveyed by the parents are shown in Table I. Regurgitation, vomiting and stool problems (25%) were the most common presenting complaints in first 2 months of life, followed by jaundice (22%) and respiratory symptoms (15%). In the age group 0-6 days, jaundice was the presenting complaint in more than half of the infants and amongst infants 7-27 days of age , jaundice was still the single most common problem (15%) though as a group, concerns about stooling, vomiting and regurgitation accounted for 25% of the visits. Stooling problems, vomiting and regurgitation were the major reasons (33%) for seeking care in the second month of life whereas respiratory symptoms like cough and noisy breathing accounted for 25% of the visits.
Table I Frequency (%) of Presenting Complaints in Infants Enrolled in the Study
Others included respiratory distress, diarrhea, constipation, cramps/colic and Vaginal problems (<1 % each). Table I shows the characteristics of the enrolled infants. Two-thirds of the infants were male and three-fourths were breast fed. A majority of the mothers had received antenatal care and delivered in a health facility. Only 5% of the infants had been born before term. Of the enrolled infants, 356 (28%) were under 7 days of age. Among those enrolled , 54 (15.1%), 35 (7.5%) and 23 (5.1%) infants in the 0-6 days, 7-27 days and 28-59 days age groups respectively were classified as having "severe illness requiring urgent hospital management" by the pediatrician. TABLE II Population Characteristics (percentages except where indicated)
* Information missing for 287/1268 (23%) of cases, #Information missing for 100/1268 (8%) of cases. For all other items percent missing was less than 3%. Amongst all the infants needing hospital management, 46% were because of jaundice while 17 % each were due to sepsis and pneumonia / lower respiratory tract infection (LRTI). The primary diagnosis for which infants required admission also varied according to the age (Table III). In the first week of life, 78% of babies were admitted because of jaundice. In the age group 7-27 days, 29% were admitted due to jaundice, an equal number had sepsis as the primary diagnosis and another 20% had pneumonia/LRTI. Amongst infants 28-59 days of age, pneumonia/LRTI was the primary diagnosis in half of the admitted infants while sepsis accounted for another 17%. TABLE III Frequency (%) of Primary Diagnoses (pediatrician assessment) by Age and Need for Hospitalization
Blood cultures were performed in 112 cases and they were positive in 28 (25%). In the 0-7 days age group, 29% of the cultures sent yielded organisms while only 19 % of the cultures were positive in 8-59 days age group. The commonest organism isolated in both age groups was Staphylococcus aureus (46%). The other isolates were Acinetobacter sp., Escherichia coli, Klebsiella pneumoniae and Enterococcus sp. TABLE IV Frequency and the Odds Ratio of Individual Signs (excluding jaundice) for Prediction of “Serious Illness” Requiring Urgent Hospital Management
The frequency of clinical signs and their odds ratio for predicting urgent hospital management in three age groups are shown in Table IV. Considering symptoms and signs with a prevalence of at least 5%, in the first week of life, a history of not feeding well (OR 14.7), and a respiratory rate >60/min (OR 21.5) were the only two significant predictors, although the individual sensitivity of each was less than 60%. In the age group 7-27 days, a history of not feeding well (OR 8.0) and a respiratory rate >60/min (OR 6.2) were the only two significant predictors, but had low sensitivities. Amongst infants 28-59 days, a history of not feeding well (OR 11.3), and a respiratory rate> 60/min (OR 10.5) continued to be significant predictors; in addition, severe chest in-drawing (OR 4.6) by itself was also a significant predictor of admission. Further analysis of the independence of the predictors and models combining multiple symptoms and signs for prediction of severe illness will be reported in a paper combining findings from all the study sites. Discussion The study aimed to assess the predictive ability of symptoms and signs of severe illness in the first 2 months of life that can be used by the ANM in the community to identify infants who need to be referred to the hospital. So, we simulated the situation in a first level health facility in the community where the infant would be first seen by the ANM/health worker. Like the Delhi center of this multi-centre study, the majority of the infants had been born in a health facility(4 ). However, only 8.8 % of the enrolled infants required admission at our site as compared to 19.6 % at the Delhi site. This was in spite of a larger proportion of infants of 0-7 days age at the Chandigarh site (28 % vs 11 %). The study showed that the predominant reasons for seeking health care in infants below 2 months of age were jaundice, feeding and stooling problems (vomiting, regurgitation, gastrocolic reflex, colic), and respiratory problems (cough, noisy breathing). The experience from Delhi site which enrolled infants from Safdarjang hospital was almost similar except for small differences in the proportions. A careful scrutiny shows that a large proportion of these presenting complaints are innocuous or physiological. Education of the parents and the community health workers regarding the management of these will help allay their anxiety and avoid unnecessary referral. Systematic information about illnesses of young infants in the community is scant (5-7). The current study quantifies the prevalence of various illnesses in the first 2 months of life, which may help in planning educational and interventional strategies . At the same time, the health worker should have access to reliable validated symptoms and signs which can be used to diagnose severe illness warranting referral. The major diagnoses requiring hospital admission were jaundice, pneumonia/LRTI and sepsis. In the first week of life, jaundice was responsible for 78% of admissions. At the Delhi site also, jaundice was the single most important reason for admission in the first week- however, it contributed to only 56% of admissions with sepsis emerging as the second commonest cause in 21%. In 7-27 days age group, jaundice and sepsis were the major reasons of admission at both the sites while pneumonia and sepsis were the commonest diagnoses amongst admissions in 8-59 days age group at both sites-the only difference was that diarrhoeal illnesses contributed to about 10% of admissions in Delhi whereas they were negligible in Chandigarh. Hence, the predictive symptoms and signs to be used by the health worker should reflect these groups of diagnoses. Also, the symptoms and signs to be used by a peripheral health worker should have reasonable sensitivity i.e. they should be occurring rarely even though they may be specific. Hence, symptoms and signs with a prevalence of at least 5% were considered to see if they significantly predict hospital admission. A history of not feeding well and a respiratory rate >60/min had significant positive predictive ability for severe illness in all the 3 age groups studied. In the second month of life, in addition, severe chest in-drawing was also a significant predictor. Although they had good specificity, the sensitivity of these three symptoms/signs was low. This implies that if used singly, they would miss many infants requiring admission. The solution to this is studying the predictive abilities of these symptoms/signs in combination, which is the subject of the multi-site analysis. At the Delhi site, apart from history of not feeding well and a respiratory rate > 60/min, fever, convulsions, lethargy and diarrhoea were also significant predictors of illness requiring admission (4). The IMCI algorithm includes a list of 14 signs and the presence of any clinical sign is considered suspicious for a serious bacterial illness (1,2,8). The IMNCI adaptation for neonates in India is also based on consensus opinion of experts. Some of the signs included in this adaptation, such as bulging fontanel, sclerema and central cyanosis, were not seen in the current study. On the univariate analysis, we found only a few signs to have significant positive predictive value and a prevalence of at least 5%. The goal of the multi-site analysis would be to find the minimum number of symptoms/signs which can reliably predict serious illness and are also seen reasonably frequently in the community. At this single site, the numbers studied may have been too small to identify some important signs. Bang et al in their home based trial in Gadchiroli, found that birth weight <2000 g, preterm birth (<37 weeks) or baby not taking feeds or mother reporting that baby's feeding has decreased at any time during 2-28 days together made a good combination to detect neonates at risk of death( 9). However, in their cohort , the incidence of sepsis was 18 % as against an incidence of 5% in our study(10 ). Also, nearly 10% of the newborns were preterm in the Gadchiroli cohort versus 5% in the study from our site. In a study from Kenya, the following were predictive of bacterial sepsis: omphalitis, prostration, hypoxemia (saturation <90%), weak or absent movements, abnormally irritable or sleepy, abnormal feeding, inability to console the infant, and bulging fontanel (11). The lack of valid clinical signs for the diagnosis of severe bacterial illness (SBI) in neonates has been also reported by Kumar and Singhi who found that a combination of two or more out of three criteria could identify 95 % of infants with SBI. However, two of these criteria involve laboratory testing which may not be feasible(12 ). Limitations of our study The studied population was a low risk population with satisfactory antenatal care. The majority of deliveries were conducted by trained persons, which is not typical for the country at large. The ANMs in the study were trained in the pilot phase and they underwent a periodic re-checking and re-training. It would remain to be seen how the skills imparted to the ANM/health worker in the community can be sustained. The number of infants less than 7 days of age was small giving rise to wide confidence intervals for the predictive symptoms and signs. This should be taken care of once the data from all sites is combined. Conclusions In this study, we documented the main reasons for care seeking in the first 2 months of life in a North Indian urban and peri-urban population. The 2 most important predictive signs for the need for hospital admission as determined from this study include a history of not feeding well and a respiratory rate >60/min. In addition, severe chest in-drawing was another significant predictor in the second month of life. In combination with the findings from other sites, an algorithm could be developed for use by less skilled health workers around the globe to detect infants requiring hospital care. This will be the basis for the refinement of the Indian IMNCI as well, which should lead to improved care and decreased mortality in this vulnerable age group. Acknowledgement The authors wish to express their gratitude to the Department of Child and Adolescent Health and Development (CAH) of WHO, Geneva ,Switzerland, for financial support, and to Dr Jose Martines for his encouragement, support and technical assistance. We would like to acknowledge the constant encouragement and guidance from Dr C P Bansal, Ex-Director Health Service, UT Chandigarh and Dr Usha Bishnoi, Medical Superintendent, General Hospital, Sector 16, Chandigarh. Contributors credit: Protocol development MW, AN; data collection PM, SM; study monitoring RN, PK, AN; microbiology PR; data analysis JBC, PG; paper writing PK, AN, JBC, MW; guarantor AN. Funding: WHO-CAH Geneva. Competing interests: None
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()