|
|
Research Paper Indian Pediatrics 2007; 44:739-748 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Clinico-epidemiological Profile and Predictors of Severe Illness in Young Infants (<60 days) Reporting to a Hospital in North India |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
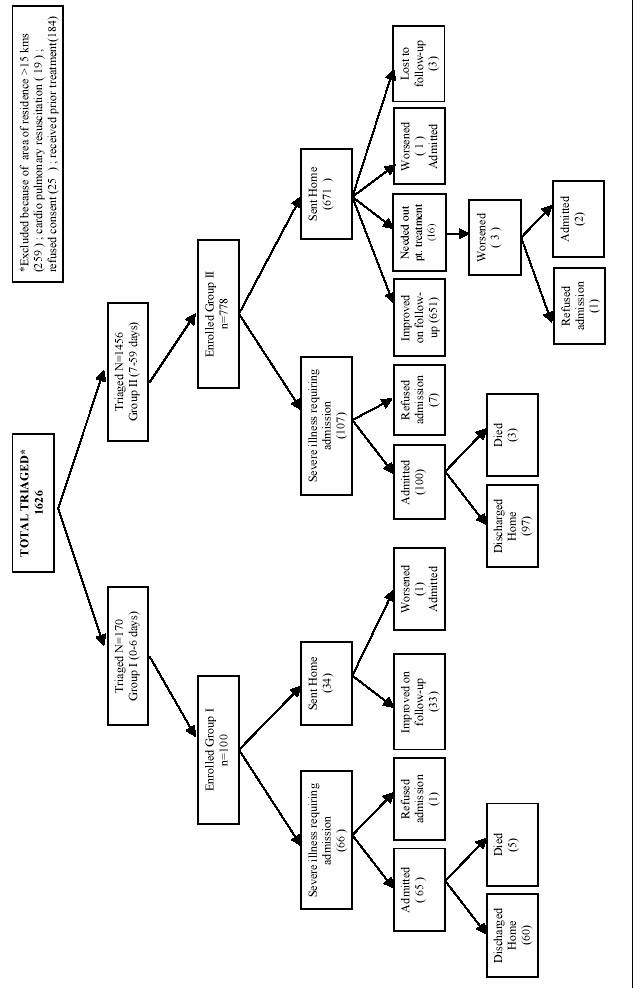
INDIA accounts for 27% of the global burden of neonatal deaths each year. Nearly two-thirds of the infant mortality and 46% of the under five mortality occurs in the neonatal period in India(1-2). It is recognized that to reduce infant and under-five mortality, health problems that occur during the first two months of life must be addressed as a high priority. Estimates of direct causes of death indicate that severe infections account for 36% of neonatal deaths (sepsis/pneumonia 26%; tetanus 7%; diarrhea 3%)(3). Three-fourths of neonatal deaths occur in the first week of life(4,5). For infants in the first week of life, in particular, little information is available on the potential value of different clinical features that might be of use to identify severe illness requiring hospital treatment. It is, therefore, of major public health importance to identify simple symptoms and signs in young infants predict severe illness warranting admission to health facility or referral for treatment. The current Integrated Management of Childhood Illnesses (IMCI) guidelines have been developed from a study performed in 4 countries looking at children with possible infection but they have not been validated in other settings. Above all, a generic IMCI algorithm has not been developed for identification and referral of serious illness warranting admission for the early neonatal period (<7 days). It is now apparent, however, that the endpoints for measurement in the young infant study (YIS) may have been too narrowly focused, without sufficient attention to non-infectious disease(6-8). While many sick young infants needing referral will have severe bacterial illness (SBI) as a major diagnostic consideration, those under 7 days of age, in particular, may need referral for increased surveillance and/or management of a variety of conditions not addressed in the YIS that may not cause the newborn to be obviously sick, such as severe jaundice, low birth weight, or poor feeding due to prematurity. Finally, the relatively small number of very young infants (i.e., 300 in the 0-6 day age range of a total of about 3300 young infants) that were enrolled limited the analysis of signs and symptoms predictive of illness in this age group. Current management guidelines for infants <7 days are based more on experience and expert opinion. This study was undertaken as part of a multi-centre study to validate the utility of the clinical signs and symptoms previously identified in the young infant guidelines for identifying ill young infants, especially those in the first week of life. The current paper reports in detail results obtained at the Delhi site of this international study designed to assess the value of simple clinical signs for helping health workers to identify young infants with severe illness warranting hospital admission. Methods This prospective study was conducted at Safdarjung Hospital located in South Delhi, in collaboration with the All India Institute of Medical Sciences, New Delhi, from May 2004 to May 2005. Safdarjung Hospital is a referral hospital which also cares for unreferred patients from the Delhi neighborhood in the outpatient department. Approximately 50,000 to 60,000 children under 5 years are seen every year. The study was preceded by a pilot phase in which the study procedures were standardized and tested using customized forms with a manual of operations. Eligible were young infants <60 days of age presenting to the outpatient department of the hospital because of illness as perceived by the mother or guardian. They were screened by a triage person for inclusion into the study. Babies were excluded if they lived further away than 15 km from the hospital (to ensure follow up), had been hospitalized in the previous 2 weeks (except for delivery) or were enrolled in the study for an earlier episode or referred from another health care facility or by a physician and specific therapy had been instituted prior to referral, or if they had an obvious lethal malformation (anencephaly, etc.), or if they required immediate cardiopulmonary resuscitation, or the guardian refused consent. Written informed consent was taken for enrollment into the study. Infants who were excluded from the study or those brought to hospital outside study hours, were referred to the emergency ward or outpatient department for further evaluation and treatment. The study enrollment was done on 4 days per week i.e., Monday, Tuesday, Thursday and Friday in two shifts (9.00 am to 9 pm) each day. Wednesdays and Saturdays were utilized for follow-up evaluation and home visits. Study procedure Young infants screened by the triage person and enrolled into the study were sent to Study person A for recording history and a selected list of pre specified clinical signs. Study person A (Staff Nurse- General Nursing) evaluated the infant using a structured form A which included details on demographic data, historical factors and signs in a standardized format. After study person A had completed her assessment, the patient was referred to study person B (a pediatrician) who was blinded to study person A’s findings. The study persons were located in different rooms and performed their examinations independently. Study person B documented signs in an unstructured format and decided on the need for urgent admission to hospital for medical reasons based on his/her clinical judgment. The training of study persons A and B was accomplished through didactic sessions and actual demonstration of clinical signs using cases and video demonstrations prepared for use at all sites participating in the study. Study person B categorized primary and secondary diagnosis using standard definitions as per the manual of operations. In order to ensure that the admission decisions by study person B were generally consistent with acceptable practices, the case histories were reviewed on an ongoing basis by the principal investigator or co-principal investigators who were senior pediatricians with >15 years experience. All enrolled patients were examined in detail. Pulse oximetry was performed after clinical examination in all infants using an Oxy 500 A pulse oximeter (Deus Infocom, USA). All those who needed admission underwent blood culture and serum glucose determination. Specific criteria were also used to identify infants for lumbar puncture. All jaundiced infants had serum bilirubin estimation by a capillary bilirubin analyzer (Cosmo Medical, Model Bil -100, South Korea). Chest X-ray was done if the admitted infant had respiratory signs. The clinical course of the infant in the hospital (i.e., condition improved, cured, left hospital against medical advice, death at the end of the hospitalization) was recorded along with the final diagnosis at discharge, taking the clinical course and the results of investigations into consideration. Procedure for infants not admitted All patients who were sent home were advised to return for re-evaluation within 48-72 hours. When the caretaker brought the child for follow-up assessment on the scheduled visit, reevaluation was done to determine whether the child was well, sick or needed hospitalization. If the caretakers of the infant did not return for follow-up on a scheduled appointment, a telephonic call was made. If she/he still did not return, a home follow-up visit was undertaken within 7 days of the initial hospital visit. At the home visit, an evaluation was done to determine whether the infant was seriously ill or if the caretaker of the infant thought that there had been deterioration since attendance. The parents were then encouraged to bring the infant to the study site for evaluation. If the patient had been admitted to another hospital, hospital details were recorded for the outcome. The filled forms A and B were reviewed by one of the senior investigators at Safdarjung Hospital and afterwards sent to the principal investigator at AIIMS. A review committee of three pediatricians reviewed 20% of all admitted and 10% of outpatient records. The comments and feedback of the review board members were conveyed to study person B. Data entry, cleaning and management Case record forms were checked for completion and correctness, and then double entered into an Epi-Data data base (V.2.1, EpiData Association, Odense Denmark, www.epidata.dk). Data files were sent to the international data coordination centre where further consistency checks were performed and the quality of data submitted from the individual sites was monitored. Statistical methods The primary analysis consisted of tabulations of the primary outcome classification and major specific diagnoses. Further analysis included univariate analysis of the association between the primary outcome (the "severe illness requiring hospital admission" classification by study person B) and individual clinical signs and symptoms, tabulation of sensitivity and specificity , and estimation of odds ratio (OR), with 95% confidence intervals (CI). In this paper we investigate the value of non-jaundice signs and symptoms, so patients admitted with a primary diagnosis of hyperbilirubinemia or physiological jaundice were included in the control ("non-admitted") group. Further analysis of predictors of hyperbilirubinemia, and of the combined sites will be reported elsewhere. Analysis was done using Stata version 8 software (Stata Corp., College Station, Texas, USA). Ethical clearance The study was approved by the Ethics Committee of the All India Institute of Medical Sciences, the WHO Ethical Research Committee and the Indian Council of Medical Research. Results A total of 1624 young infants were triaged, of whom 878 cases satisfied the criteria for enrollment into the study. The study flow is provided in Fig. 1. Reasons for exclusion were: residing >15 km from study site 259; needed immediate resuscitation 19; received prior treatment 184; refused consent 25. Of the enrolled children, 100/878 (11%) were below 7 days of age. Most of the babies were born in a health facility (90%), received antenatal care (95%), were delivered by skilled birth attendants (91%) and were born at term (88 %). Baseline clinical characteristics of the enrolled cohort are given in Table I.
TABLE I Baseline Clinical Characteristics of Study Group (percentages except where indicated)
* Information missing for 185/878 (21%) of cases; for all other items percent missing was less than 2%. TABLE II Frequency (%) of Presenting Complaints in Infants Enrolled in the Study
(Others includes infrequent complaints cramps, irritable, abdominal distension, vaginal problems, jitteriness, small baby, urinary problem , paralysis (<2%).
Reasons for seeking care are presented in Table II. Sixty-six of 101 (66%) neonates in the first week of life (of whom one refused admission), and 107/778 (13.8%) of the older triaged infants, seven of whom refused admission, were sick enough for hospitalization. Table III provides details of the primary clinical diagnoses categorized on infant's age and need admission. The most frequent primary diagnosis in the age group <7 days needing admission to hospital was hyperbilirubinemia (56%), followed by sepsis (21%); in those between 7-27 days it was sepsis (27%) and in the age group 28-59 days of age it was pneumonia (40%) and sepsis (19%). Ten infants with serious illness (5 with sepsis; 3 with diarrhea, and dehydration; 1 with Downs’ syndrome; 1 with hyperbilirubinemia) left against medical advice. Although, eight were well after leaving the hospital, two could not be traced. There were eight deaths: 5 in the age group <7 days (sepsis two; immaturity one; epidermolysis bullosa one; kernicterus one) and 3 in age group 7-59 days (meningitis one; sepsis one; aspiration one). TABLE III Frequency (%) of Primary Diagnoses (pediatrician assessment) by Age and Need for Hospitalization
Of the 705 babies who did not require admission, nearly all (except 3) were followed after 2-4 days. Most (683/705) returned for follow up as per study protocol but 48 babies (6%) required home visits. Only 12 babies required further follow up and in four babies admission was advised on first follow up examination. Of these two got admitted and two refused admission but improved on outpatient treatment (study flow). None of them died. TABLE IV Frequency and the Odds Ratio of Individual Signs for Prediction of “Serious Illness” Requiring Urgent Hospital Management
0-6 days: Information was missing for 1-2% of cases for the following signs: Not feeding well, History of no cry at
birth, History of feeding problem since birth.
7-27 days: Information was missing for 11% of cases for the sign “History of no cry at birth”, and for 1-2% of cases
for: History of difficulty feeding, Not feeding well, History of feeding problem since birth.
28-59 days: Information was missing for 12% of cases for the sign: “History of no cry at birth”, and for 2% of cases
for: “Not feeding well”.
The frequency of clinical signs and their odds ratio for predicting urgent hospital management in three age groups are shown in Table IV. Looking at symptoms and signs with a frequency of at least 5%, for the age group <7 day, a history of feeding difficulty (OR 6.5), not feeding well on observation (OR 19.4), a temperature >= 37.5ºC (OR 5.6), a RR >= 60 (OR 36.8) and history of convulsions (OR 32.1) emerged as the most important symptoms and signs for predicting the need for admission. In older neonates aged 7-27 days, a number of individual signs clustered as general (history of fever OR 2.8, history of difficult feeding OR 13.1, not feeding well OR 23.3, lethargy OR 26.1, and temperature >37.5ºC OR 13.1); respiratory (respiratory rate >60/min OR 18.5), diarrhea (history of diarrhea OR 2.5) were found to be significant. In young infants 28-59 days of age, individual symptoms and signs clustered as general (history of fever OR 4.0, history of difficult feeding OR 6.2, not feeding well OR 20.9, and temp >37.5ºC OR 30.0); respiratory (respiratory rate >60/min OR 36.1) were found to be significant. Further analysis of independent predictors and combination models for prediction rules will be reported in a summary paper combining findings from all the study sites. Blood cultures were performed in 122 of 165 admitted cases (including 60 babies with neonatal hyperbilirubinemia). Culture was positive in 25 (21%), the commonest organisms isolated being Enterobacter and Staphylococcus aureus (26.6%) each. The other isolates were Acinetobacter sp., Escherichia coli, Citrobacter sp., Klebsiella pneumoniae and Enterococcus sp. Discussion We studied signs of severe illness in a suburb of Delhi, where the population had good access to health care, antenatal care and institutional delivery. In this setting, common reasons for care seeking were jaundice, not feeding well and fever in neonates 0-6 days of age; and respiratory symptoms in older infants 7-59 days of age. Reasons for care seeking are different in other settings, for example in Chandigarh it was predominantly jaundice, feeding, stooling (vomiting, regurgitation, gastrocolic reflex, colic) and respiratory problems (cough, noisy breathing)(10). Severe illnesses among young infants need to be identified early by health workers so that early case management can be instituted in a health facility. For infants aged 7-59 days the guidelines are based more on research and the results of a previous WHO multi-center study while for infants <7 days the evidence for recommendations are scanty and are therefore based more on experience and expert opinion. The IMCI criteria include a list of 14 signs and the presence of any clinical sign is considered to be suspicious for a serious bacterial illness(11). The current IMNCI algorithm for neonates in India is again based on the consensus opinion of experts. We could show at the Indian sites that there are small number of key signs adding little by themselves to prediction rule, as they are often associated with other, more common signs. From a training and retention of knowledge perspective, they are difficult to teach, as they are infrequently seen. We, therefore, stressed signs in the univariate analysis with at least 5% prevalence. However, all signs were included in the multivariate analysis in the summary paper to explore their significance (submitted for publication). Despite their significant contribution to child mortality, diseases in young infants in developing countries are rarely reported from community settings and secondary health facilities(12-14). The current study provides a new and informative descriptive background on the characteristics of young infants reporting to secondary health facility in North India. A number of clinical symptoms and signs in young infants especially in age group 7-59 days were predictors of severe illness warranting admission to hospital. These are general (history of fever, difficult feeding, not feeding well, and temperature >37.5ºC); respiratory (respiratory rate >60/min), neurological (history of no cry at birth), diarrhea (history of diarrhea). Individual signs taken alone in isolation had a very high specificity but limited sensitivity. This indicates that an algorithm with a constellation of signs can be worked out to have acceptable levels of sensitivity and specificity so as not to miss serious illness needing admission or referral, while avoiding too much over referral. For neonates below 7 days of age, a single sign, either not feeding well on observation or even history of not feeding well, had an acceptably high sensitivity and specificity in predicting the need for hospital admission. In this population we did not encounter sclerema, central cyanosis, bulging fontanelle. In clinical practice this has to be weighed in relation to teaching of health workers who have to be trained to pick a manageable number of signs. A simpler algorithm than the existing IMCI requiring only limited signs easily recognizable by health workers and not requiring laboratory testing would be useful in practice, if it has acceptable sensitivity and specificity. The concurrent Chandigarh study showed major reasons for hospital admission as jaundice, pneumonia/LRTI and sepsis(10). History of not feeding well and respiratory rate >60/min had significant predictive ability in all three age groups. In Gadhchiroli home based trial, retrospective analysis of clinical criteria for at risk neonates of death on first day of life indicated that birth weight <2000 g, preterm birth (<37 weeks) or baby not taking feeds or mother reporting that baby’s feeding has decreased at any time during 2-28 days together make a good combination(15). In another study from Kenya, which included infants in the neonatal period, the following were predictive of bacterial sepsis: Omphalitis, prostration, hypoxemia (saturation <90%), weak or absent movements, abnormally irritable or sleepy, abnormal feeding, inability to console the infant ,and bulging fontanels (16). The lack of valid clinical signs for the diagnosis of severe bacterial illness (SBI) in neonates has been also reported by Kumar and Singhi: None of the signs they studied in a hospital setting predicted SBI satisfactorily, while only the combination of two or more out of three criteria could identify 95 percent of infants with SBI. However, two of these criteria involve laboratory testing which may not be feasible in resource restricted countries(17). The present study has the limitation that it included a relatively small number of babies in age group <7 days, resulting in less precision of estimates. Moreover, most of the babies were born in the hospital delivered by skilled attendants. This may imply that these neonates were from surrounding semi urban areas belonging to a relatively higher socio-economic status. Conditions like asphyxia or sick babies specially those with birth weight <1500 g who succumb in the early days of life were selectively not included. These issues will be taken care in the summary paper which provides information from six countries with varied population of enrolled young infants from community sites at Pakistan to first level health facilities at Bolivia and South Africa. The current study is based on a population of young infants reporting to a health facility avoiding selection bias of hospital admitted sick infants as was the case in earlier studies. As such, limited data have been published from India on the clinical characteristics and predictors of severe illness in young infants requiring hospital management. Such data are needed to design improved prospective evaluation of possible case management strategies and refine clinical practice guidelines for IMNCI in the country. Acknowledgements The authors wish to express their gratitude to the Department of Child and Adolescent Health and Development (CAH) of WHO, Geneva, Switzer-land, for financial support, and to Dr Jose Martines for his encouragement, support and technical assistance. We would like to acknowledge contributions of Dr Rakesh Lodha, Assistant Professor and Dr Shinjini Bhatnagar, Research Scientist in the Department of Pediatrics at the All India Institute of Medical Sciences, New Delhi for agreeing to be on the review board for validating decisions of the pediatrician about the need for admission. This study would not have materialized without constant encouragement and guidance from Dr R N Salhan , Medical Superintendent, Safdarjung Hospital, New Delhi. Contributors credit: Protocol development MW, VKP, JBC; data collection SV, JS, RJ; study monitoring AKD, HC, MSP, DKT, PP; microbiology AK; data analysis JBC, PG ; paper writing AKD, VKP, JBC, MW; guarantor AKD Funding: WHO-CAH Geneva. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()