|
|
Research Papers Indian Pediatrics 2007; 44: 732-736 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Serum Interleukin-18 Levels are Raised in Diabetic Ketoacidosis in Chinese Children with Type 1 Diabetes Mellitus |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Genetic predisposition to develop Insulin dependent type 1 diabetes mellitus (T1DM). T1DM may contribute to the preferential production in "high risk" individuals of large amounts of type 1 pro-inflammatoy cytokines such as interleukin (IL)-1, IL-2, IL-12, IL-18 and interferon (IFN)-g that stimulate cellular effectors of DTH responses (T cells, macrophages, NK cells)(1,2). Particular attention has been focused on the role of IL-1 beta, IL-12, and IFN-g as these cytokines are also capable of directly influencing beta cell function and viability in vitro(3). Recent studies have reported that an up-regulated production of IL-18 could be an important pathogenic event in the dysregulated production of IFN-g and other type 1 cytokines thought to predispose to immunoinflammatory disease such as T1DM(7-9). Moreover, the potential role of IL-18 in the pathophysiology of the chronic complications of diabetes mellitus has also been reported(7-11). However, data are very limited for the IL-18 potential role in the acute complications such as diabetic ketoacidosis (DKA). In the present study, we compared serum IL-18 levels as well as other cytokines (IL-12 and IFN-g) among newly diagnosed T1DM with DKA, T1DM without DKA and 30 age and sex-matched healthy controls. Subjects and Methods The study population consisted of Group 1 : 28 children with T1DM and DKA; Group 2 : 33 children with T1DM, but no DKA; and Group 3 : 30 healthy children without T1DM or family history of diabetes. Diagnosis of T1D and DKA was made as per standard recommendations(12,13). Characteristics of these 3 groups of children are compared in Table 1. All patients and controls or their parents were informed of the purpose of the study, and their written consents were obtained. TABLE I Characteristics of Enrolled Subjects
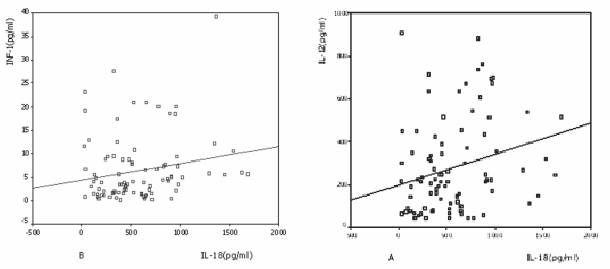
* p <0.01, ** p <0.05 None of the subjects suffered from infectious, allergic or other autoimmune diseases in the 6 months before sampling, and they did not use immunomodulatory drugs in the 3 months preceding the study. Venous blood was collected from all subjects between 9.00 and 10.00 a.m. to minimize possible circadian variations. Blood specimens were allowed to clot at room temperature and the sera were immediately separated by centrifugation at 1000/min and stored at –70ºC until assayed. The cytokines IL-18, IL-12 (p40), IFN-g were measured by the same person on research ELISA plates (DIACLONE, France) according to the instructions supplied by the manufacturer and met the quality assurance and quality control established for test validity. The intra-assay and inter-assay coefficients of variations (CVs) were 6.1% and 6.5% for IL-18, 5.0% and 6.0% for IL-12, 4.9% and 10% for IFN-g, respectively. Detection levels were 45 pg/mL for IL-18, 20 pg/mL for IL-12 and 5 pg/mL for IFN-g respectively. Statistical analyses were conducted by using SPSS software (version 10.0). Pearson chi-square was used to measure the enumeration data between subgroups. Quantitative data were presented as mean ± SD. Because the data for IL-18, IL-12, and IFN-g were not normally distributed, they were transformed logarithmically. The statistical significance between means was estimated by an independent-samples t test. Differences were considered statistically significant at P <0.05. Results The characteristics of control subjects and patients with T1DM are shown in Table 1. Serum IL-18 levels were significantly higher in patients than those in age- and sex-matched controls (692 ± 381.4 pg/mL vs. 310.0 ± 265.3 pg/mL, P = 0.03). However, the serum IL-12 and IFN-g levels were not different between patients and controls (277.5 ± 207.0 pg/mL vs351.4 ± 223.4 pg/mL, P = 0.446 and 7.0 ± 7.5 pg/mL vs 5.6 ± 5.3 pg/mL, P = 0.215, respectively). We found a significant correlation between serum IL-18 and ICA (r = 0.219, P =0.035) and C-peptide levels decreased (r = – 0.249, P = 0.016), but we could not find significant correlation between serum IL-18 and HbA1C, insulin and glucose (all P>0.05) in T1DM. Serum IL-18 levels also correlated positively with serum IL-12 levels (r = 0.254, P = 0.014) (Fig. 1).
Serum IL-18 levels was significantly higher in patients with DKA than those in patients without DKA (IPI = 0.001) while C-peptide levels were markedly lower in patients with DKA (P = 0.033). On the other hand, IL-12, IFN-g and other biochemical markers, such as TC, TG and HbA1C were not statistically different between two groups (all P >0.05). Discussion Our results demonstrated that serum IL-18 levels were significantly higher in patients with T1DM than in age-and sex-matched control subjects, which is consistent with previous studies(8,9). That IL-18 could play a part in the pathogenesis of type 1 diabetes mellitus is also supported by in vivo studies in NOD mouse model of type 1 diabetes showing that IL-18 is required for the development of destructive insulitis and diabetes(4,14). In the present study, we found that serum IL-18 levels correlated positively with serum IL-12 levels and tended to correlate positively with serum IFN-g levels. It has been reported that IL-18 acts synergistically with IL-12 to increase the amount of IFN-g produced by Th-1 cells and also induces IFN-g production by NK cells(15). Generally accepted concepts of the development of T1DM indicate that the pathogenic contribution of IL-18 occurs through its ability to stimulate T-cell synthesis of IFN-g. Subsequently, when the production of IFN-is sufficiently upregulated, the cytokine could itself become capable of sustaining its own increased production by stimulating IFN-g producing T cells. This could in turn potentiate and prolong the type 1 cytokine profile observed at the onset of T1DM which is characterized by increased circulating levels of IFN-g, IL-12 and IFN-g. We could not found significant correlation between serum IL-18 and HbA1C, a measure of average blood glucose concentration during the preceding 6-8 weeks in the diabetic patients. One possible explanation is that the hyperglycemic clamp study showed serum IL-18 concentrations rising to a peak at 2 h and retuning to basal levels at 3h in diabetic patients(16). Moreover, we showed that serum IL-18 levels were positively correlated with ICA, a mixture of various autoantibodies binding to islet cell cytoplasm constituents in cryostat sections of human pancreas. C-peptide levels are the most reliable factor evaluating the endogenous insulin secretion in patients with T1DM, even who has presented with DKA(17). We found that C-peptide levels were decreased in T1DM with DKA and IL-18 levels were negatively correlated with C-peptide levels. These associations of islet autoantibody status, C-peptide levels and serum IL-18 levels provides further evidence for the clinical relevance of systemic concentrations of autoimmune b-cell destruction. Our data also showed that serum IL-18 levels were significantly higher in patients with DKA than those in patients without DKA. IL-18 can activate lymphocyte ability and lead to production of other proinflammatory molecules, such as IL-8, IFN-g and IFN-1b from mononuclear cells and macrophages. These molecules are known to increase in DKA with T1DM (18). This suggested that IL-18 might play a role in the occurrence of DKA in patients with T1DM children. In conclusion, the present results indicate that serum IL-18 levels are elevated and correlated with C-peptide levels and ICA in patients with T1DM, with marked increase in T1DM with DKA. Practitioners treating type 1 diabetes mellitus should be aware of the risk of diabetic ketoacidosis in diabetic patients with high serum IL-18. Acknowledgements We thank all the children and their parents for participating in this research project. We thank Drs. Wang Chunlin, Hong Fang and Jiang Youjun for their exceptional patient care and organization. We also thank Chen Liqin for her assay expertise. Contributors: DGP: concept of study, study design and manuscript drafting. LL: analysis of data and revising of the manuscript. FJF and ZCC: data collection and analysis. GDP will act as guarantor of the study. Funding: Supported by the Bureau of Science and Technology of Zhejiang province (No: 2005C33027). Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()