|
|
Case Reports Indian Pediatrics 2005; 42:1033-1036 |
||||||
|
CSF Rhinorrhea and Recurrent Meningitis Caused by Transethmoidal Meningoencephaloceles |
||||||
|
From the Departments of Radiology & Imaging and Pediatrics*, University College of Medical Sciences & GTB Hospital, Dilshad Garden, New Delhi 110 092, India. Correspondence to: Professor Satish K. Bhargava, Department of Radiology and Imaging, University College of Medical Sciences & GTB Hospital, Dilshad Garden, New Delhi 110 092, India.
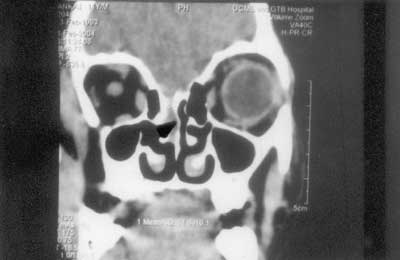
Cerebrospinal fluid (CSF) Rhinorrhea is commonly caused by trauma involving the floor of the anterior cranial fossa with tearing of the duramater. Rarely, congenital defects in the skull base associated with cephaloceles(1) can result in CSF rhinorrhea. We report two children with CSF rhinorrhea and recurrent meningitis in whom the diagnosis of transethmoidal meningoencephalocele was made by multislice CT without the use of any contrast. Case Report Case 1 An 11-year-old boy presented with complaints of nasal discharge off and on since last 1 year. The discharge increased on bending the head down, coughing and sneezing. During this period there were three episodes of high-grade fever, requiring hospitalization. There was a past history of fall from height at the age of 1 year with bleeding from the nose. The intervening period of 8-year following trauma were uneventful. With a provisional diagnosis of CSF rhinorrhea with recurrent meningitis, a non-contrast multislice spiral CT scan of the paranasal sinuses was performed. The CT scan showed a defect in the cribriform plate of the ethmoid bone on the left side (Fig. 1a). A mass showing mixed soft tissue and fluid attenuation was seen herniating through the defect into the left ethmoid sinuses and nasal cavity. (Fig. 1b). The frontal lobe was also seen herniating downwards through the defect. Multiplanar reconstruction allowed us to delineate the bony defect and soft tissue mass better. (Fig. 2). MRI with MR Cisternography confirmed the diagnosis of transethmoidal meningoencephalocele.
The child underwent endonasal endo-scopic ethmoidectomy. The left middle turbinate was resected. Brain tissue was found protruding from the cranial cavity between the middle and superior turbinate laterally and perpendicular plate of ethmoid bone medially. Anterior ethmoidectomy was done. A defect was found in the olfactory fossa. The protruding brain tissue was cauterized and removed. The defect was repaired with a graft harvested from the right conchal perichondrium along with surgical gel. Post- operatively the child was put on anti-convulsants prophylactically. Lumbar puncture catheter was inserted in subarachnoid space to decrease CSF pressure and removed after 4-5 days. The child was asymptomatic on follow up after 2 months. Case 2 A 12-year-old boy presented with recurrent pyogenic meningitis and rhinorrhea comprising clear watery fluid from the right nostril off and on since the last 3 years. There was no past history of trauma. A multislice spiral non-contrast CT scan showed a large defect measuring 1.4 × 0.7 cm in the right cribriform plate. A mass with fluid density was seen herniating through the defect into the posterior ethmoid sinus along with the right frontal lobe. A diagnosis of congenital transethmoidal meningoencephalocele was made which was later confirmed on MRI. The child underwent a right frontal craniotomy, which showed a defect at the base of the frontal lobe with brain matter herniating down. This was excised and the defect closed with pericranium graft and surgical gel foam. Discussion Cephaloceles are congenital herniations of intracranial contents through a defect in the cranium and duramater. If the herniation contains only meninges it is a meningocele When the herniation contains brain along with meninges it is known as meningo-encephalocele. Transethmoidal encephalo-celes are rare(2) constituting less than 10% of all encephaloceles(3). It is a rare cause of CSF rhinorrhea and recurrent meningitis. The transethmoidal defects lie anteriorly either along the midline or along the cribriform plate and do not involve the sella turcica. The hernial sac extends inferiorly into the sinuses or nasal cavity and typically contains portions of frontal lobes and olfactory apparatus. Tranethmoidal encephaloceles most commonly present with recurrent episodes of meningitis(2), intermittent CSF rhinorrhea(4) or sometimes as a nasal mass. The infant or child can present with unilateral nasal obstruction, chronic nasal discharge or headache after forceful blowing of nose(4). They are easily misdiagnosed as nasal polyps and this can be potentially fatal after erroneous polypectom(4). Therefore, imaging studies should always be obtained in patients with polypoidal nasal lesions prior to biopsy. Associated congenital anomalies like mid face anomalies, orbital malformations or hydrocephalus may be present. Besides the typical clinical history the diagnosis of CSF rhinorrhea was made by invasive investigations e.g., Radioisotope cisterno-graphy(3). It involved injection of radioactive tracer into the lumbar CSF, with wool pledgets placed in the roof of both nasal cavities and subsequently measuring radioactivity in the pledgets to indicate the anatomic location of leak. A simpler method was to place Dextrostix in the various sites to look for the glucose in CSF(5). The presence of a positive 2-transferrrin band in the immunological tests performed on the nasal fluid proved particularly helpful in diagnosing CSF rhinorrhea(4). However, with the advent of multislice spiral CT and its capability of multiplanar reconstructions a non-contrast CT scan can non-invasively display the osseous defect beautifully in cases of CSF rhinorrhea. MRI has a superior soft tissue resolution. It can define the nature of the cephalocele and allow an accurate depiction of the olfactory and optic tracts, hypothalamic-pituitary system associated agenesis of corpus callosum when present(1). MR cisternography can also be done without intravenous contrast. In our cases multi-slice CT was able to make the diagnosis of transethmoidal meningoencephalocele non-invasively in both the children, without the use of any contrast. Three-dimensional multiplanar reconstruc-tions with CT allowed a more precise description of the bony defect than MRI. This is essential for surgery. However, MRI allows the best description of herniating meninges, brain or ventricles as well as associated cerebral anomalies(1) without the use of ionizing radiation. Thus imaging studies such as CT and MRI should be obtained in patients of recurrent meningitis with CSF rhinorrhea. Contributors: PG carried out the radiological work up, collected the clinical data and reviewed the literature. PG and VR drafted the manuscript. SKB and VR critically reviewed the manuscript. AA was responsible for the clinical work up of the cases. Funding: None. Competing interests: None stated. | ||||||
|
References | ||||||
|
|
![]()