|
|
Case Reports Indian Pediatrics 2001; 38: 1181-1184 |
||||
|
Primary Immature Mediastinal Teratoma in a Newborn |
||||
|
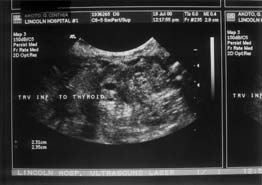
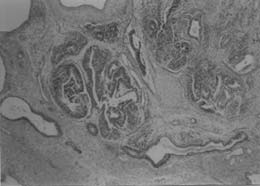
Primary immature mediastinal teratoma is very rare. In newborn period, these tumors can cause life threatening respiratory obstruction and must be promptly diagnosed and treated if the patient is to survive. In this report, the clinical course and histopatho-logical findings of immature teratoma in a newborn is described. This case is noteworthy as an example of immediate postnatal respiratory distress due to space occupying nature of an immature mediastinal teratoma with normal chest X-ray findings. Case Report A preterm (35 weeks), appropriate for gestational age, male infant was born by vaginal delivery to a 36-year-old mother (G2 P1) who had regular antenatal examinations during pregnancy. The mother was admitted 2 days before delivery because of pregnancy induced hypertension. An abdominal sono-gram on admission revealed polyhydramnios. Magnesium sulphate therapy was adminis-tered for pre-ecclampsia and the maternal serum magnesium level was 8 mg/dl. Apgar score of the newborn was four, six and seven at one, five and ten minutes, respectively. The neonate required resuscita-tion with positive pressure ventilation using an ambu bag. He was admitted to NICU and was placed in an incubator on 25% oxygen by nasal canula. Physical examination revealed moderate respiratory distress, marked by grunting and intercostal and subcostal retractions. The initial arterial blood gas (ABG) in 25% FiO2 showed pH of 7.20, pCO2 of 48 Torr and PO2 of 86 Torr. Nasal continuous positive airway pressure (NCPAP) with 5 cm of H2O was given to the baby. The serum magnesium level was 10 mg/dl. Over the first 20 hours the infant appeared unstable with varying respiratory effort and oxygen requirement. At 20 hours of life oxygen saturation dipped to 69% and he was intubated. Followed intubation, respiratory distress dramatically improved. A chest radiograph taken at this time was normal. The neonate was examined by the otolaryngology service and laryngomalacia was ruled out. Patient was extubated at 40 h of life at which time the serum magnesium level was 4.1. At 48 hours of life respiratory distress recurred with cyanosis and decreased air entry in both lung fields. ABG in room air showed pH of 7.07, pCO2 of 103.9 Torr and pO2 of 74.7 Torr. He was re-intubated and, again, immediately following intubation, his respiratory status improved greatly and oxygen saturation increased dramatically. At that time, a 3.0 ´ 2.0 cm firm mass was palpated in supra-sternal region, which increased in size on crying. Ultrasound revealed a 3.0 ´ 2.5 cm heterogeneous mass separate from the thyroid gland and the mass was highly vascular on Color Doppler study (Fig. 1). CT scan showed the mass extending from neck into the mediastinum and confirmed its heterogeneous consistency. A differential diagnosis of thymoma versus teratoma of the anterior mediastinum was considered. The pediatric surgeon was consulted. The neonate was operated on day five. The mass was completely excised from the anterior mediastinum via median sternotomy. Histopathologic examination of the mass revealed a mixture of epithelial and mesenchymal tissue; immature neuroglial and neuroectodermal elements constituting about 50% of the tumor. Based on the morphology a diagnosis of immature teratoma was made (Fig. 2). The infant remained asymptomatic and was discharged home on day 15 of life. At present, he is well and symptom-free at 6 month follow-up.
Discussion Mediastinal teratomas are uncommon in infants and children, constituting 7% to 10% of all teratomas in this age group(1,2). In newborns, immature teratomas are rare and constitute less than 1% of all mediastinal teratomas. Other uncommon sites where im-mature teratomas are reported in early infancy include brain(3), neck(4), pharynx(5), stomach(6) and mesentery(7). Review of literature revealed that respiratory distress is the most common presentation of immature teratoma of mediastinum in newborn(2,3,8). Chest X-ray often demonstrated a mediastinal mass, some of which are calcified, but a definite diagnosis of teratoma is established only after microscopic examination(2). In the present case the initial respiratory depression was thought to be due to hypermagnesemia. Since the initial physical examination and chest X-ray were normal, an extrinsic obstruction to upper airway was not suspected until the neonate was intubated with immediate relief of symptoms. Immature teratoma is characterized by the presence of elements that resemble embryo-nic tissues, including neuroglial or neuro-epithelial components that may coexist along with mature tissues. In most instances, immature teratomas occurring in the fetus and newborn are associated with a favorable prognosis(1,8,9). The behavior of immature teratoma in adolescents and adults is less predictable and may be associated with poor clinical outcome(8). Dehner cites a 15% overall malignancy rate for mediastinal teratomas diagnosed in the pediatric age group(1). However, other workers concluded that the mediastinal teratomas, both mature and immature, occurring in newborns and infants behave in a benign fashion, if resectable, and are associated with a favor-able prognosis as compared to those occurring in adolescents and adults(2,8,10). In our case complete surgical excision of the tumor was possible through a median sternotomy. As per the available literature, this patient is expected to have a benign clinical course in spite of large areas showing immature elements. The current case highlights the symptoms of fluctuating upper airway obstruction secondary to an immature mediastinal teratoma in a newborn in whom the initial examination and normal chest X-ray were misleading. The mediastinal mass, which was compressing the trachea and esophagus, was the cause of polyhydramnios, an association reported in literature. We suggest that, mediastinal tumor though a rare cause of respiratory distress in newborn period should be considered in the differential diagnosis. Acknowledgement We thank to Dr. Karl Schultze, Depart-ment of Pediatrics, New York Presbyterian Hospital, Columbia University Medical Center for the critical review of the manuscript. Contributors: BD collected the data and drafted the paper; CR and RL helped in data collection and review of literature; SS reviewed the pathology slides, prepared the microphotographs and revised the paper.
Funding:
None.
References
|
| 1. Dehner LP. Gonadal and extragonadal germ cell neoplasia in childhood. Human Pathol 1983; 14: 493-511. 2. Lakhoo K, Boyle M, Drake DP. Mediastinal teratomas: Review of 15 pediatric cases. J Pediatr Surg 1993; 28: 1161-1164. 3. Pinto V, Meo F, Loiudice L, D’ Addario V. Prenatal sonographic imaging of an immature intracranial teratoma. Fetal Diagn Ther 1999; 14: 220-222. 4. Dunn CJ, Nguyen DL, Leonard JC. Ultrasound diagnosis of immature cervical teratoma: A case report. Am J Perinatol 1992; 9: 445- 447. 5. Mcmohan MJ, Chescheir NC, Kuller JA, Wells SR, Wright LN, Nakayama DK. Peri-natal management of a lingual teratoma. Obstet Gynecol 1996; 87: 848-851. 6. Sarin YK, Agarwal LD, Jhamaria VN, Goyal RB, Sharma R, Shekhawat NS. Immature gastric teratoma. Indian J Pediatr 1997; 64: 896-898. 7. Marcolongo A, Divirgilio G, Bettili G, Savero CF, Fasoli L, Marradi P, et al. Immature mesenteric teratoma in a male newborn infant: Prenatal ultrasonographic diagnosis and surgi-cal treatment. Prenat Diagn 1997; 17: 686-688. 8. Carter D, Bibro MC, Touloukian RJ. Benign clinical behavior of immature mediastinal teratomas in infancy and childhood; Report of two cases and review of the literature. Cancer 1982; 49: 398-402. 9. Isaacs H Hr. Perinatal (Congenital and neonatal) neoplasms: A report of 110 cases. Pediatr Pathol 1985; 3: 165-216. 10. Tapper D, Lack EE. Teratomas in infancy and childhood: A 54-year experience at the Children’s Hospital Medical Center. Ann Surg 1983; 398-410. |