|
|
Original Articles Indian Pediatrics 2001; 38: 1099-1105 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Successful Management of Infantile Hypertrophic Pyloric Stenosis with Atropine Sulfate |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Manuscript received:
October 20, 2000, Initial review completed: November 14, 2000,
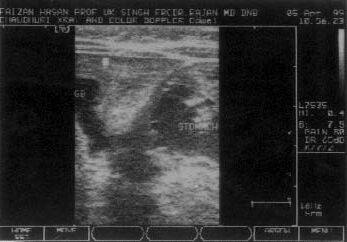
ALTHOUGH Infantile Hypertrophic Pyloric Stenosis (IHPS) has been described since eighteenth century, the present day knowledge is about 100 years old (1897)(1). Early in the twentieth century the mortality rate of this condition was about 50% irrespective of the mode of treatment(1,2). Beginning with gastrojejunostomy, the treatment journey of this condition came to a halt with the introduction of a surgical procedure called Fredet-Ramstedt operation in 1912 and till date is universally considered as the treatment of choice. Meanwhile occasional trials of medical management for this condition using methyl scopolamine nitrate(3) and atropine sulfate(4) were reported but were not enough to strengthen their claim as another treatment option. So we conducted a clinical trial using atropine sulfate aided by ultrasonic monitoring to determine the efficacy of medical manage-ment of this condition. Subjects and Methods The study period was from February 1995 to January 1999 and included 52 confirmed cases of IHPS hospitalized at Child Care Center, Patna (India). Parents were explained the purpose of the trial and written consent was obtained. The diagnosis was made clinically followed by barium meal and ultrasonography to confirm the diagnosis, rule out pylorospasm and assess the degree of severity of the condition. All patients were free of any other disease. Treatment began with correction of electrolyte imbalance and dehydration using appropriate fluids and intravenous atropine sulfate at a dose of 0.06 mg/kg/day in eight divided doses. Each dose was given very slowly (over 2 minutes) and the mother of the baby was persuaded to feed her baby at least 20 minutes after the injections. Amount and type of feed was not restricted initially. The dose was increased by 0.015 mg/kg/day till vomiting ceased and remained so for 24 hours at a stretch and ultrasound also showed a transit time of less than 1 minute. Patients requiring more than two weeks of intravenous treatment received only restricted amount of 5% glucose solution. Control of vomiting for 24 hours with intravenous atropine was followed by ultrasonic evaluation of the transit time of gastrict contents through the pyloric canal. During the initial stages of our study (including first five patients), oral atropine was started as soon as patient became and remained free of vomiting for 24 hours without taking into account the transit time. But out of five, three patients began to vomit within a day of oral treatment, which however, was controlled by increasing the oral dose by ¼th of it’s strength daily till vomiting ceased and remained so for 24 hours. On careful examination it was found that vomiting recurred in only those patients who at the end of intravenous treatment had a transit time of more than one minute. The other two who made uneventful recovery had a transit time well short of 1 minute. So further on (from patient 6 onwards), transit time was assessed daily after cessation of vomiting with intravenous atropine and oral atropine was started only when both criteria, i.e., vomiting free status for 24 hours and transit time of less than 1 minute were satisfied. Oral atropine was given at double the effective intravenous dose in eight divided doses at least 20 minutes before feeds. After 48 hours of oral treatment at hospital, patient were discharged on the same dose and feeding schedule. Oral treatment was given for three weeks. At the end of oral treatment, repeat ultrasonic evaluation of the pyloric muscle was done in every patient and same was done at 3, 6, 9, 12 and 15 months follow up to check the regression in the hypertorphy. Ultrasonographic assessment of the thickness of the pylorus was done by measuring the distance of the hypoechoic area between the submucosa and the outer margin of the muscle. Length of the pyloric canal was then assessed by measuring the distance between the pyloric and duodenal end. During hospitalization, heart rate, temperature and body weight was monitored daily while liver function and renal function was tested on the 4th day of treatment and repeated only if found abnormal. In the event of abnormal LFT or renal function and tachycardia the dose was not increased and feeds were restricted to 5% glucose solution. Results The details of patient characteristics and response to therapy are depicted in Table I. A dramatic reduction in frequency of vomiting was observed in all 52 patients within 24 hours of treatment. Twenty five patients with initial ultrasonic evidence of mild hyper-trophy (thickness/length = 3 to 5.5 mm/ 16.5 to 19.4 mm) became vomiting free after 1-3 days of intravenous atropine therapy. Dose of intravenous atropine required by these cases to remain vomiting free for 24 hours ranged from 0.06 mg/kg/day to 0.09 mg/kg/day. In 16 out of these 25 patients, cessation of vomiting was also associated with a transit time of less than one minute. The oral dose of atropine in these 16 patients ranged from 0.12 mg/kg/day to 0.18 mg/kg/day. Eight out of these 25 patients required one additional day of intravenous treatment to bring their transit time below 1 minute. The effective intra-venous dose in these eight patients ranged from 0.09 mg/kg/day to 0.105 mg/kg/day. Dose of oral atropine given to these 8 patients ranged from 0.18 mg/kg/day to 0.21 mg/kg/day. One patient (Case 2) with mild hypertrophy required 0.09 mg/kg/day of intravenous atropine to remain vomiting free for 24 hours after which he was straightaway given oral atropine at 0.18 mg/kg/day without taking into account the transit time. Vomiting recurred in this patient within a day of oral treatment which was controlled only after increasing the oral dose to 0.27 mg/kg/day. Sixteen patients with initial ultrasonic evidence of moderate hypertrophy (thickness/length - 5.6 to 8 mm/19.5 to 22.4 mm) became and remained free of vomiting after 4-7 days of intravenous treatment. Dose of intravenous atropine required for this ranged from 0.105 mg/kg/day to 0.15 mg/kg/day. In 10 out of these 16 patients, ceasation of vomiting was also associated with a transit time of less than one minute. The oral dose of atropine sulfate in these 10 patients ranged from 0.21 mg/kg/day to 0.3 mg/kg/day. Five of these 16 patients required one additional day of intravenous treatment to bring their transit time below 1 minute. The effective intravenous dose in these 5 patients ranged from 0.135 mg/kg/day to 0.165 mg/kg/day. Dose of oral atropine received by these 5 patients ranged from 0.27 mg/kg/day to 0.33 mg/kg/day. One patient (Case 5) with moderate hypertrophy became and remained vomiting free with 0.135 mg/kg/day of intravenous atropine and as has been mentioned earlier, the transit time was not taken into account and oral atropine was started straightaway at a dose of 0.27 mg/kg/day. Vomiting recurred in this patient also within a day of oral treatment which was controlled only after increasing the oral dose to 0.473 mg/kg/day. Nine patients with initial ultrasonic evidence of severe hypertrophy (thickness/length = 8.1 to 9.4 mm/22.5 to 26 mm) required 8-12 days of intravenous treatment to become and remain vomiting free for 24 hours. Dose of intravenous atropine required for this ranged from 0.165 mg/kg/day to 0.225 mg/kg/day. In 3 of these 9 patients, cesation of vomiting was also associated with a transit time of less than 1 minute. The dose of oral atropine sulfate in these patients ranged from 0.36 mg/kg/day to 0.45 mg/kg/day. Five of these 9 patients required two additional days of intravenous treatment to bring the transit time below 1 minute. The effective intra-venous dose in these 5 patients ranged from 0.225 mg/kg/day to 0.255 mg/kg/day. Dose of oral atropine given to these patients ranged from 0.45 mg/kg/day to 0.51 mg/kg/day. One patient (case 3) with severe hypertrophy became and remained free of vomiting with 0.165 mg/kg/day of intravenous atropine and as has been mentioned, was given oral atropine at 0.33 mg/kg/day without taking the transit time into account. This patient also began to vomit within a day of oral treatment. Vomiting in this patient was controlled by increasing the oral dose to as high as 0.66 mg/kg/day. All these 50 patients except three (cases 2,3 and 5) made uneventful recovery during and after oral treatment. The three afore-mentioned patients also made uneventful recovery after their vomiting was controlled with revised oral dose. Two patients (Case 8 and 49) with initial ultrasonic evidence of severe hypertrophy continued to vomit at least once every day even after two weeks of intravenous treatment and ultimately opted for plyoromyotomy. Ultrasonic evidence of normalization of pylorus was observed 3 to 15 months (Mean ± SD = 9.42 + 3 months) after completion of oral treatment. Figures 1-4 illustrate the serial changes in ultrasono-graphy with treatment. Apart from mild tachycardia in 3 patients and slight increase in SGPT in 8 patients, none of the other patients experienced significant side effects.
Discussion Atropine sulfate is an anticholinergic drug with strong antimuscarinic effects. The fact that atropine sulfate was effective in 96.2% and almost effective in remaining 3.8% cases, indicates that acetylcholine plays a significant role in the pathophysiology of IHPS. As none of the medically treated patients relapsed after completion of medical treatment, the basic defect must have been rectified either by atropine or spontaneously during the course of treatment. Because vomiting was con-trolled long before resolution of hypertrophy and the relevant antimuscarinic effect of atropine is control of spasm produced by acetylcholine, the basic defect could be none or underproduction of endogenous neuro-transmitters which antagonize the action of acetylcholine, e.g., Nitrous Oxide (No.) and Vasoactive Intestinal Polypeptide (VIP)(5,6). Normalization of endogenous production of these neurotransmitters during the course of atropine therapy could be the reason behind non-relapse in many of these patients. However, variation in the effective dose of atropine could be due to variations in the endogenous production of neurotransmitters, subjective differences in the sensitivity of muscarinic receptors and drug delivery and clearance system. Initially atropine was given intravenously because orally it would not have reached it’s site of absorption, i.e., intestine. Oral atropine was not given till transit time of gastric contents through the pyloric canal went below 1 minute because desirable amount of atropine might not have reached the intestine in time to produce effect, the reason obviously being over dilution with gastric contents and delayed emptying. Oral atropine was given at double the effective intravenous dose because in adults it has been shown that oral dose of atropine is double of effective intravenous dose(7). Oral atropine was continued for 3 weeks to ensure sufficient production of endogenous neurotransmitters, though we could not deduce the optimum duration of oral treatment. Ultrasonography (USG) is a reliable tool for confirmation of diagnosis, measurement of thickness and length of canal and demonstration of passage of gastric contents through pyloric canal(8,10). Although there are no reports regarding classification of IHPS, we tried to classify the cases as mild, moderate and severe on the basis of initial USG findings, only for the convenience in our study. Patients with thickness less than 5.5 mm were grouped as mild, those with less than 8 mm and more than 5.5 mm were grouped as moderate and those with more than 8 mm were grouped as severe cases. The fact that 50 out of 52 patients were cured and had normalization of pylorus with atropine sulfate, speaks volumes about the effectiveness of this treatment option. Even in those two patients who opted for pyloro-myotomy after two weeks of intravenous treatment, the frequency of vomiting was reduced to one episode per day and perhaps a bit longer trial might have avoided the surgery. Surgical correction of this condition is no doubt very effective but so may be atropine sulfate. Cost and duration of hospital stay with medical treatment is very much within affordable limits. Besides, pyloromyo-tomy is associated with risk (11,13) like perforation of duodenal mucosa, wound infection, wound dehiscence, gastroenteritis, post operative pyrexia and the risk of anesthesia. No such risk is involved with atropine sulfate treatment. Normalization of pylorus takes 2-12 weeks(14) with surgery, while in our study it took 3-15 months. However, presence of a symptomless hyper-trophied pylorus for a limited period of time may not have much clinical significance. In conclusion, in this series atropine sulfate proved effective, cheap and safe treatment option for IHPS. However, further confirmatory trials are required before atropine sulfate can be considered as an alternative therapeutic modality for this condition. Acknowledgment We are thankful to Dr. A.K. Patwari, Dr. Jagdish Prasad Sharma, Dr. Rajan Choudhary and Dr. Uday Krishna who helped in critical appraisal of the manuscript. Contributors: UKS and RK co-ordinated the study and drafted the manuscript. UKS will act as the guarantor for the paper. SS participated in data collection and co-drafted the manuscript. Funding: None.
References
|
|
|
![]()