A 12 year old female child was admitted with generalized convulsions.
Following recovery, she developed loss of speech, loss of vision and
mental obtundation. She also had gradually increasing severe pin-prick
like pain in lower limbs, right more than left, for last 2 months. She was
a known case of nephrotic syndrome, diagnosed 5 years back and had been
treated from elsewhere irregularly with long continued steroids at varying
doses without remission. Her mid-thigh circumference 5 cm above knee joint
was 26 cm (right) and 28 cm (left). The femoral pulse volumes were feeble,
the right more than the left. There was a discernible temperature
difference between the right lower limb and other parts of the body. The
blood pressure in both upper limbs was160/100mmHg. It was 104/50 mm Hg in
right lower limb and 168/132 mm Hg in the left lower limb. There were a few
ulcerative lesions over both thighs. The skin over the right lower limb
was thin, atrophic and shiny with loss of hair. Hemoglobin, leucocyte and
platlet count and erythroytic sedimentation rate, and cerebrospinal fluid
were non-contributory. Urinalysis showed an albuminuria of ++++, plenty of
red cells and pus cells 5-8/HPF. Sera for ANA, anti dsDNA, pANCA, cANCA,
APLA (IgG&IgM) and HBsAg were non-reactive. There was gross derangement in
lipid profile. Both her parents had normal lipid profile.
CECT brain revealed venous infarct in right cerebellar
hemisphere and right temporoparietal cortex. Color doppler study of lower
limbs revealed extensive atherosclerotic plaque of both lower limbs with
vascular compromise, right more than the left. All arteries in the lower
limbs, extending from abdominal aorta to dorsalis pedis showed features of
gross atherosclerotic changes. No feature suggestive of deep venous
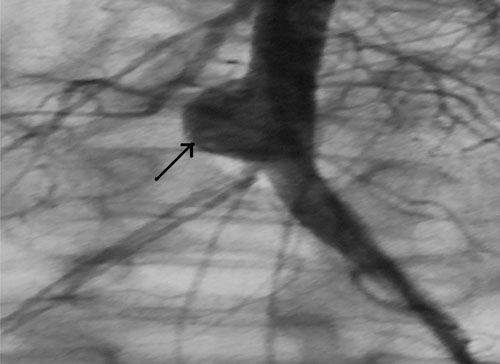
thrombosis was detected. Angiography of abdominal aorta and lower limb
vessels corroborated the doppler findings. It also revealed a large
aneurysm at the bifurcation of the common iliac vessels (Fig. I).
Angiography of coronary arteries was within normal limits. Renal biopsy
suggested advanced stage of focal segmental glomerulosclerosis (FSGS).
 |
|
Fig.1 Angiography of lower limb vessels
showing atherosclerotic obstruction and aneurysm formation (black
arrow) |
There are a few case reports of premature coronary
atherosclerosis in steroid resistant nephrotic syndrome in children [1,2].
But, atherosclerotic blockage of limb vessels in a child with nephrotic
syndrome has not been reported before. Diagnosis was more in favour of
atherosclerosis of lower limb vessels rather than thrombotic episode
because she had symptoms relating to the vascular insufficiency in lower
limbs for more than two months before presenting to us. There were also
skin lesions suggesting chronic vascular insufficiency. Moreover, aneurysm
formation is more likely to be associated with atherosclerotic vascular
insufficiency rather than thrombosis. Both Doppler USG and angiography
were in favour of atherosclerosis. Hyperlipidemia is an integral component
of nephrotic syndrome [3] but the long term implications of this fact in
children is not known. The role of statins needs to be explored [4,5].
Reference
1. Kallen RJ, Brynes RK, Aronson AJ, Lichtig C, Spargo
BH. Premature coronary atherosclerosis in a 5-year-old with
corticosteroid-refractory nephrotic syndrome. Am J Dis Child.
1977;131:976-80.
2. Hopp L, Gilboa N, Kurland G, Weichler N, Orchard TJ.
Acute myocardial infarction in a young boy with nephrotic syndrome: a case
report and review of the literature. Pediatr Nephrol. 1994;8:290-4
3. KuŸma E, Roszkowska-Blaim M. Lipids abnormalities in
children with refractory nephrotic proteinuria [Article in Polish] Przegl
Lek. 2006;63: Suppl 3:201-4.
4. Sanjad SA, al-Abbad A, al-Shorafa S. Management of
hyperlipidemia in children with refractory nephrotic syndrome: the effect
of statin therapy. J Pediatr. 1997;130:470-4.
5. Querfeld U. Should hyperlipidemia in children with
the nephrotic syndrome be treated? Pediatr Nephrol. 1999;13:77-84.


