|
|
|
Indian Pediatr 2009;46: 933-938 |
 |
Two Doses of Measles Vaccine Reduce Measles
Deaths |
|
Maya van den Ent, Satish Kumar Gupta and Edward Hoekstra
Correspondence to: Maya van den Ent, Health Specialist,
UNICEF, 3 UN Plaza, New York, USA.
Email: [email protected]
|
|
Abstract
Two doses of measles vaccine to children reduce
measles related deaths. The first dose is delivered through the routine
immunization system to infants and the 2nd dose through campaigns or
routine immunization system, whichever strategy reaches the highest
coverage in the country. Experience in 46 out of 47 measles priority
countries has shown that measles vaccination using mass vaccination
campaigns can reduce measles related deaths, even in countries where
routine immunization system fails to reach an important proportion of
children. The gradual adoption of this strategy by countries has
resulted in 74% reduction in measles related deaths between 2000 and
2007. The 2010 goal to reduce measles mortality by 90% compared with
2000 levels is achievable if India fully implements its plans to provide
a second dose measles vaccine to all children either through campaigns
in low coverage areas or through routine services in high coverage
areas. Full implementation of measles mortality reduction strategies in
all high burden countries will make an important contribution to
achieving Millennium Development Goal 4 to reduce child mortality by two
thirds in 2015 as compared to 1990.
Key words: Measles, Mortality, Supplemental immunization
activities, Two dose strategy.
|
|
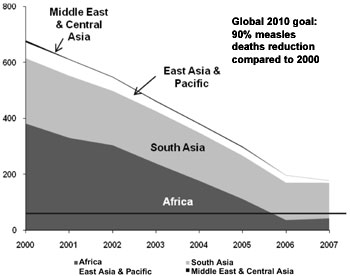
The introduction of a second dose for
measles vaccination using mass vaccination campaigns…,
along with improved routine immunization, has averted an estimated 3.4
million measles deaths between 2000 and 2007 in countries with previously
high measles burden. In the last nine years, 46 out of 47 countries with
more than 95% of the global measles deaths in 2000, introduced a 2nd
chance for measles vaccination, resulting in 74% reduction of measles
deaths between 2000 and 2007. Impressive progress was made in the African
region by 2006 and sustained in 2007, where measles deaths were reduced by
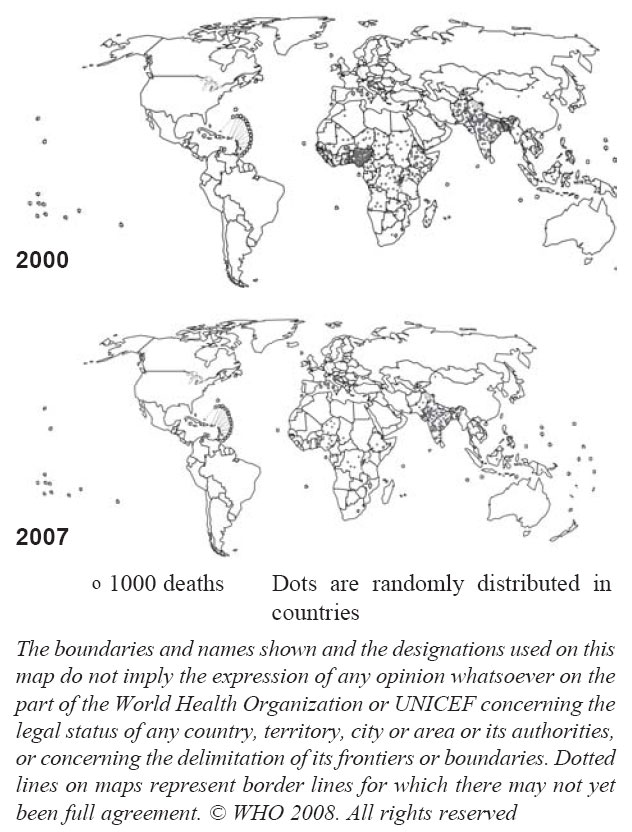
89% from 395,000 in 2000 to 45,000 in 2007(1,2) (Fig.1&2).
|
 |
|
Fig. 1 Estimated measles death, 2000-2007 per region(1,2).
|
|
|
|
Fig. 2 Distribution of 750,000 estimated measles
deaths, 2000 and 2007(1,2).
|
In November 2008, the Strategic Advisory Group of
Experts (SAGE) on immunization has recommended that all children should
receive two doses of measles containing vaccine: the first dose during
routine vaccination program and the second dose either through routine
services or through mass campaigns (SIAs) …,
depending on which strategy achieves the higher coverage(3-5). This is an
important change to the previous recommendation that one dose of measles
containing vaccine would be sufficient to control measles.
As of 2009, all but one country has adopted a two dose
strategy for measles control. India is currently in the process of
introducing the 2nd dose of measles vaccination in their childhood
vaccination program. This is important, as one out of six people live in
India and an estimated 123,000 child deaths annually could be averted by
offering timely two doses of measles vaccine to Indian children(1,2).
Measles Kills
Measles is one of the most contagious viral diseases
and affected almost every child before widespread use of the measles
vaccine. About 6 million measles related deaths were estimated to occur
globally each year before the use of the live attenuated measles vaccine,
licensed in 1963(6). Although measles deaths in industrialized countries
are rare, measles is often fatal in developing countries with increased
risk of deaths for children under 5 years of age, those living in
overcrowded conditions, who are malnourished (especially with vitamin A
deficiency), and those with immunological disorders, such as advanced HIV
infection(7,8). Measles infection leads to immune suppression in the host,
lasting for up to one month, that reduces patients’ defenses against
complications such as pneumonia, diarrhea, and acute encephalitis.
Pneumonia, either a primary viral pneumonia or a bacterial
super-infection, is a contributing factor in about 60% of measles-related
deaths(7,8).
Globally, measles case fatality rates (CFR) vary widely
among countries, regions, age and within the same community in different
years. Higher CFRs occur in outbreaks, among children under 5 years of
age, in secondary cases, in cases with complications, and in unimmunized
individuals. Vaccination is associated with milder disease(7,8). Sudfield
and Halsey reviewed the CFRs of 25 studies in Indian communities,
presented elsewhere in this issue (mean CFR = 4.27%, range 0.00% - 31.25%,
median = 1.63%, range 0.00% - 31.25%). This review reveals that CFR
decreased over time, probably due to higher vaccination coverage. In
addition, children living in rural areas are more at risk of dying from
measles than those living in urban settings(9).
Control Strategies
After the introduction of measles vaccine in the
routine immunization program, along with improved nutrition, living
conditions and case management, measles related annual deaths reduced to
an estimated 2.5 million by 1980(10). As a result of the increase in
coverage with the 1st dose of measles to 72% in 2000, as compared to 16%
in 1980(11), a further substantial reduction in measles mortality was
achieved. Starting in the 1990s, an increasing number of countries
introduced a second dose of measles vaccine in their routine program, as
reported to WHO and UNICEF joint reporting system. The Pan American region
provided a second dose for measles in supplementary immunization
activities that resulted in the elimination of measles by 2002 in that
region (i.e. the region had no indigenous cases, as distinct from
imported cases, for more than 12 months)(12).
Despite these results, in 2000, measles was still the
leading cause of vaccine preventable deaths in children and the fifth
leading cause of death from any cause in children under five years
old(13). Responding to this situation, in 2001, the American Red Cross,
UNICEF, the United Nations Foundation, the CDC, and WHO launched the
Measles Initiative aimed at reducing the death rate from measles in
Africa, where nearly 60% of measles deaths were occurring(14). In 2004,
the Initiative extended its mandate to other regions (notably, Asia) where
measles was a significant burden. WHO and UNICEF identified 47 high-burden
countries for priority action. ……
All these countries had low coverage
of the measles first routine dose (with an average coverage of 58%) and
offered only one dose of measles vaccine to their children in 2000.
The Initiative adopted the WHO-UNICEF strategy to
reduce measles mortality (3-5,15) that is based on the experience in the
Americas:
• achieving high coverage of the first measles
containing vaccine (MCV1) in infants
• offer a second dose through campaigns (SIAs …)
or offer in the routine program reaching very high coverage;
• laboratory backed surveillance of new measles cases
to detect outbreaks and monitor progress; and
• enhanced case management, including vitamin A
supplementation.
Failure of Routine System to Reach Children
In the 47 high burden countries for measles ……,
the routine vaccination program reached on average only 58% of the infants
in 2000. Although the coverage increased to 72% in those countries by
2007, adding a 2nd dose to this weak program would not have resulted in a
significant increase of population immunity, as an important part of the
children are missed by the routine health delivery system. Therefore, a
different strategy was adopted to reach previously missed children and
increase population immunity.
In countries where the system fails to reach a large
part of the children, the only effective delivery system to reach over 95%
of the children nationwide is mass vaccination campaigns. Therefore,
offering the second dose through a campaign is the preferred strategy to
ensure sufficient children are protected from measles to significantly
reduce outbreaks. In the measles priority countries, an average of 28% of
children have not received their first dose of measles vaccination before
their first birthday in 2007, and in Niger, Chad, Somalia and Laos, more
than half of the children are missed through the routine system.
In 2007, 23 million infants did not receive the 1st
dose of measles vaccination. Two thirds of them live in eight countries:
India (8.5 million), Nigeria (2.0 million), China (1.0 million), Ethiopia
(1.0 million), Indonesia (0.9 million), Pakistan (0.8 million), DRC (0.6
million) and Bangladesh (0.5 million)(11).
Catch-up Campaigns in Areas With Poor Routine Immunization Coverage
Measles catch-up campaigns have been conducted in 46 of
the 47 priority countries that adopted the strategy and vaccinated all
children aged 9 months through 10-14 years, depending on the epidemiology
of the country ….
The impact of the campaigns has been overwhelming with over 90% reduction
in measles cases, and across Africa, many hospitals have closed their
measles wards.
Subsequently, every 2-4 years follow-up campaigns have
been conducted to administer the second measles dose to children born
after the previous campaign. The frequency of the follow-up campaigns
depends on the coverage of the routine immunization. Generally, major
outbreaks can be avoided by conducting follow-up campaigns before one
birth cohort of susceptible is reached.
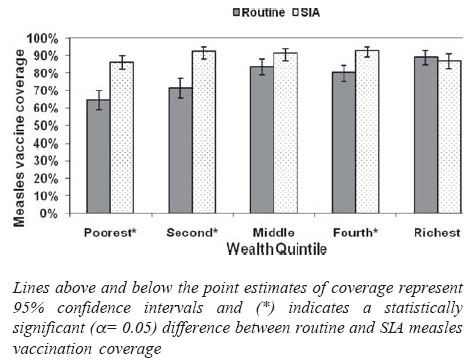
Well organized campaigns reach children across all
wealth quintiles evenly, whereas routine immunization program tends to
reach fewer children in the poorest quintiles. In Kenya, routine
vaccination reached 65% [95% CI: 59%-70%] of the children of the poorest
quintile, whereas 89% of the richest children were reached [95% CI:
85%-93%]. During the campaign the coverage was evenly distributed among
all wealth quintiles(16)(Fig.3). This indicates that
campaigns reach the unvaccinated children, including those from poorest
families.
|
 |
|
Fig. 3 Nationwide
measles vaccination coverage among children aged 9-23 months through
routine vaccination immunization programme and SIA…,
Kenya 2002(16)
|
 |
|
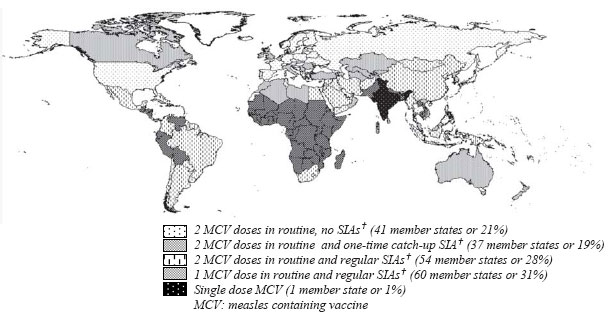
Fig. 4 Measles vaccination delivery
strategies, 2008. |
Realizing that measles is a more dangerous disease in
malnourished children and those living in overcrowded conditions, the
campaign approach seems an appropriate strategy to ensure that the poorest
children are reached and protected against measles.
Recently, countries have been organizing periodic
intensified routine immunization services or Child Health Days, where
routine immunization services, including measles vaccination, are offered
in underserved areas, often together with other life saving interventions.
This strategy has been adopted, as the number of un-immunized children
stagnated in recent years at more than 20 million. While health systems
take many years to develop and expand, extra outreach sessions can ensure
that the poorest children are also protected against vaccine preventable
diseases.
Integration
Measles vaccination has offered an excellent platform
to deliver other life saving interventions to the children, such as long
lasting insecticide treated nets, vitamin A, de-worming tablets, and polio
vaccines. Since 2001, the Measles Initiative with other partners has
supported the distribution of more than 37 million long lasting
insecticide treated nets for malaria prevention, 81 million doses of
de-worming medicine, more than 186 million doses of vitamin A, and more
than 95 million polio vaccines. Of the 33 countries conducting measles
SIAs in 2008, 29 (88%) integrated at least one other child survival
intervention with measles vaccination.
Two Dose Vaccination Schedules for Measles
To date, countries have adopted a delivery approach for
measles vaccine according to the capacity of their health system to reach
high population immunity. To stop transmission of measles virus, 93-95%
population immunity is needed, that requires a two dose schedule, as
vaccine efficacy after a single dose varies between 85 and 95%, depending
on the age at vaccination(5).
Countries with strong health systems deliver 2 doses in
the routine system only (41 of the 198 countries) or provide 2 doses
during the routine, in addition to having conducted a one- time catch-up
campaign (37 countries). Fifty-four countries provide two doses of measles
vaccines in the routine, and regularly conduct campaigns. Sixty countries
provide one dose of measles vaccination in the routine and conduct regular
campaigns. Finally, India has plans to begin introduction of a second dose
of measles vaccines in the near future (Fig.4).
Importantly, there are countries in each of the
categories that have successfully stopped measles transmission through
achieving and maintaining very high coverage with their delivery strategy,
with the exception of settings which use a single measles dose delivery
only.
According to the latest SAGE recommendations, it is
beneficial for countries to introduce a 2nd measles dose as part of the
routine vaccination programme, if the health system is sufficiently strong
and has reached at least 80% of the infants with the first measles dose
during 3 consecutive years. To ensure sufficient population immunity,
campaigns should be continued until the 1st and 2nd routine measles dose
reached 95% of the eligible children(4).
Conclusions
Significant reduction of mortality due to measles is
achieved by offering two doses of measles vaccines to all children. So
far, 46 of the 47 priority countries have adopted this strategy, further
reducing the measles related deaths by 74% between 2000 and 2007. In these
countries, all children are now offered two doses of measles vaccine, one
in the routine program and a second through campaigns by renewed delivery
strategies to reach previously unreached communities, besides closely
monitoring disease burden. Two of the 46 countries (Vietnam and Indonesia)
with stronger health systems have recently also started introducing 2nd
dose of measles in the routine immunization system.
Based on the experience in 46 out of 47 priority
countries, the 2010 goal to reduce measles mortality by 90% compared with
2000 levels(17) is achievable, if India fully implements its plans to
provide a second dose measles vaccine to all children either through
campaigns or through routine services. Full implementation of measles
mortality reduction strategies in all high burden countries will make an
important contribution to achieving Millennium Development Goal 4 to
reduce child mortality by two third in 2015, as compared to 1990.
Acknowledgments
The authors are grateful to Mickey Chopra, Maya
Vijayaraghavan, Maria Otelia Costales and Rouslan Karimov for their
contributions to the document and presentation of the data.
Funding: None.
Competing Interests: None stated.
Note: Authors are staff members of UNICEF. The
views expressed herein are those of the authors and not
necessarily reflect the views of UNICEF.
† Campaigns or
supplementary immunization activities (SIAs) are generally carried out
using 2 approaches. An initial, nationwide catch-up SIA targets all
children aged 9 months to 14 years; it has the goal of eliminating
susceptibility to measles in the general population. Periodic follow-up
SIAs then target all children born since the last SIA. Follow-up SIAs are
generally conducted nationwide every 2–4 years and target children aged
9-59 months; their goal is to eliminate any measles susceptibility that
has developed in recent birth cohorts and to protect children who did not
respond to the first measles vaccination.
††
The 47 measles priority countries are: Afghanistan,
Angola, Bangladesh, Benin, Burkina Faso, Burundi, Cambodia, Cameroon,
Central African Republic, Chad, Côte d’Ivoire, Democratic Republic of the
Congo, Djibouti, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Ghana,
Guinea, Guinea-Bissau, India, Indonesia, Kenya, Laos, Liberia, Madagascar,
Mali, Mozambique, Myanmar, Nepal, Niger, Nigeria, Pakistan, Papua New
Guinea, Republic of the Congo, Rwanda, Senegal, Sierra Leone, Somalia,
Sudan, Timor-Leste, Togo, Uganda, Tanzania, Vietnam, Yemen, and Zambia.
References
1. World Health Organization. Progress in global
measles control and mortality reduction, 2000-2007. Wkly Epidemiol Rec
2008; 49: 441-448.
2. Centers for Disease Control and Prevention. Progress
in Global Measles Control and Mortality Reduction, 2000-2007. MMWR 2008;
57: 1303-1306.
3. World Health Organization. Meeting of the
immunization Strategic Advisory Group of Experts, November 2008-
conclusions and recommendations. Weekly Epidemiol Rec 2009; 84: 1-16.
4. World Health Organization. Meeting of the
immunization Strategic Advisory Group of Experts, April 2009- conclusions
and recommendations. Wkly Epidemiol Rec 2009; 84: 213-236.
5. World Health Organization. Measles vaccines: WHO
position paper. Wkly Epidemiol Rec 2009, 84: 349-360.
6. Clements CL, Hussey GD. Measles. In: Murray
CJL, Lopez AD, Mathers CD, eds. Global Epidemiology of Infectious
Diseases. Geneva: World Health Organization; 2004.
7. Perry RT, NA Halsey. The clinical significance of
measles: a review. J Infect Dis 2004;189 (Suppl 1): S4-S16.
8. Wolfson LJ, Grais RF, Luquero FJ, Birmingham ME,
Strebel PM. Estimates of measles case fatality ratios: a comprehensive
review of community-based studies. Int J Epidemiol 2009, 38: 192-205.
9. Sudfield CR, Halsey NA. Measles case fatality ratio
in India; a review of community based studies: Indian Pediatr 2009; 46:
983-989.
10. Plotkin S, Orenstein W, Offit P. Vaccines, 5th ed.
Philadelphia: Saunders; 2008.
11. World Health Organization. United Nations
Children’s Fund. WHO/UNICEF review of national immunization coverage,
1980-2007. Geneva, Switzerland: World Health Organization; 2008. Available
at http://www.who.int/immunization_monitoring/routine/immunization_
coverage/en/index4.html. Accessed 20 September, 2009.
12. de Quadros CA, Andrus JK, Danovaro-Holliday MC,
Castillo-Solórzano C. Feasibility of global measles eradication after
interruption of trans-mission in the Americas. Expert Rev Vaccines,
2008; 7: 355-362.
13. Stein CE, Birmingham M, Kurian M, Duclos P, Strebel
P. The global burden of measles in the year 2000–a model that uses
country-specific indicators. J Infect Dis 2003;187 Suppl 1: S8-S14.
14. Wolfson L, Strebel P, Gacic-Dobo M, Hoekstra EJ,
McFarland JW, Hersh BS. Has the 2005 measles mortality reduction goal been
achieved? A natural history modelling study. Lancet 2007; 369: 191-200.
15. World Health Organization. United Nations
Children’s Fund. Measles mortality reduction and regional elimination
strategic plan 2001-2005. Geneva, Switzerland: World Health Organization;
2001. Available at http://www.who.int/vaccines-documents/docspdf01/www573.pdf.
Accessed 20 September, 2009.
16. Vijayaraghavan M, Martin RM, Sangrujee N, Kimani GN,
Oyombe S, Kalu A, et al. Measles supplemental immunization
activities improve measles coverage and equity: Evidence from Kenya.
Health Policy 2007; 83: 27-36.
17. World Health Organization. Global immunization
vision and strategy 2006-2015. Geneva, Switzerland: World Health
Organization; 2005. Available at http://www.who.int/vaccines-documents/docspdf05/givs_final_en.pdf.
Accessed 20 September, 2009.
|
|
|
 |
|
