|
|
|
Indian Pediatr 2009;46: 1017-1020 |
 |
An Outbreak of Pertussis in Sarli Circle of
Kurung-kumey District, Arunachal Pradesh, India |
|
T Takum*…,
D Gara…, H Tagyung…
and MV Murhekar*
From *Field Epidemiology Training Programme (FETP),
National Institute of Epidemiology (ICMR), Chennai;
…Directorate of
Health Services, Government of Arunachal Pradesh; and ‡General Hospital,
Naharlagun,
Arunachal Pradesh, India.
Correspondence to: Manoj Murhekar, National Institute of
Epidemiology, R-127, Tamil Nadu Housing Board, Ayapakkam, Ambattur,
Chennai 600 077, India.
Email: [email protected]
Manuscript received: February 9, 2009;
Initial review: March 2, 2009;
Accepted: March 30, 2009.
Published online: 2009 July 1.
PII: S097475590900086-2
|
|
Abstract
An outbreak of suspected pertussis occurred in Sarli
circle of Kurung-kumey district of Arunachal Pradesh in 2007. We
investigated this outbreak to confirm the etiology, estimate the
magnitude and identify reasons for its occurrence. Twenty-six deaths
were reported from the circle. We identified 72 case-patients meeting
the case definition of suspected pertussis. The overall attack rate was
30%. None of the under-five children surveyed had received any vaccine
in the past. It is essential to establish facilities for conducting
routine immunization in Sarli and organizing special campaign in the
area to vaccinate all under-fives with full course of vaccines.
Keyword: Arunachal Pradesh, Children, India, Outbreak,
Pertussis.
|
|
P
ertussis,
an acute infectious disease caused by Bordetella pertussis, remains
a major health problem in developing countries with an estimated 294,000
deaths in 2002(1). India reported 26,044 pertussis cases in 2005(1).
In late July 2007, health authorities of Kurung Kumey
district of Arunachal Pradesh reported 30 deaths from Sarli circle
(administrative sub-division) of the district with respiratory symptoms.
Director of Health Services, Arunachal Pradesh constituted a rapid
response team consisting of a pediatrician, a microbiologist and an
epidemiologist. The team could reach the affected area only after 10 days
because of incessant rains. The objectives of outbreak investigation were
to (i) confirm etiology, (ii) estimate the magnitude, (iii)
identify reasons for its occurrence, and (iv) formulate
recommendations for preventing future outbreaks.
Methods
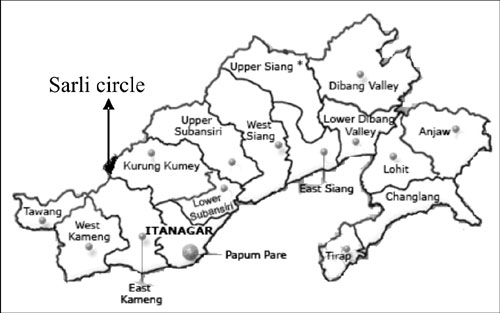
Sarli is situated near Indo-China border under newly
created Kurung Kumey district (Fig. 1). There is no road
connection to this remote outpost and it is a two days walk from the
district headquarters. In 2007, Sarli circle had a population of 2471,
residing in 26 villages. The population of these villages ranged from six
to 213. All villages are spread out and farthest village is three days
walk from Sarli. Bangro, Nishing and Sulung tribes inhabit
the area.
 |
|
Fig. 1 Location of Sarli circle, Arunachal
Pradesh, India. |
We collected the line-list of individuals who died
during the outbreak, prepared by sub-center health workers. As it was not
possible to visit all villages, we established a 24-hour medical camp at
Sarli and sent out messages to all village chiefs to bring the children
who suffered or were suffering from respiratory illness. We defined a
suspected case of pertussis(2,3) as occurrence of cough lasting at least 2
weeks with at least one of the following: (i) paroxysms of coughing
(ii) inspiratory whooping, and (iii) post-tussive vomiting;
among under-five children residing in Sarli circle since April 1, 2007. We
interviewed parents who brought their children at the camp to ascertain
the presence of symptoms and clinically examined all children. From
children meeting the case definition, we collected information about age,
sex, place of residence, date of occurrence of paroxysmal cough and
immunization status. We also interviewed parents of 18 children who died
due to suspected pertussis and who attended the medical camp with their
other children, to authenticate the information about actual deaths.
Oral, gingival and throat swabs from case-patients were
collected and sent to Regional Medical Research Center, Northeastern
Region (ICMR), Dibrugarh for microbiological investigations.
We hypothesized that the outbreak was due to low
coverage of pertussis vaccine. In absence of any data regarding
vaccination coverage in Sarli circle, vaccination status of all children
aged 12-60 months attending the medical camp was assessed. We described
the outbreak over time through an epidemic curve, constructed an area map
to describe its spatial distribution and calculated attack rates of
suspected pertussis by age and sex.
Results
During the 10 days period (6-15 August, 2007), 236
patients (122 under-fives) attended medical camp with different medical
ailments. 72 (59%) of 122 under-fives met the case definition of suspected
pertussis. There were 30 reported deaths. Of these, 26 were among
under-fives, including 15 infants. Overall attack rate of suspected
pertussis was 30% (Table I). Median age of case-patients was
26 months (range, 3–60 months).
Besides cough of
³2-weeks
duration, common clinical features of 72 case-patients identified in
medical camp were paroxysms of coughing (100%), post-tussive vomiting
(100%), inspiratory whooping (1.3%), tearing of frenulum of tongue (4.2%)
and sub-conjunctival hemorrhage (1.3%). No pathogen could be isolated from
the samples sent for microbiological investigations. None of the suspected
case-patients could undergo X-ray evaluation to rule out pneumonia.
 |
|
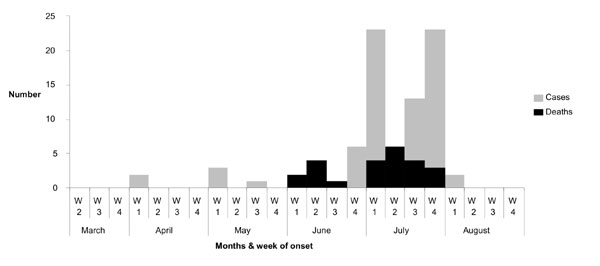
Fig. 2 Epidemic curve of suspected
pertussis cases and deaths by week of onset, Sarli circle, Kurung
Kumey district, Arunachal Pradesh, India, 2007. |
Attack rates of suspected pertussis were higher among
infants (71%), females (40%) and among Sulung tribe (40.4%) (Table
I). Cases started occurring from 1st
week of April 2007 and reached a peak during July 2007 (Fig. 2).
Cases were reported from 12 of the 26 villages (data not shown). None of
the 122 under-fives who attended the medical camp had received any primary
vaccination.
TABLE I
Incidence of Suspected Pertussis, Arunachal Pradesh, India, 2007
|
Demographic Characteristics |
Population*
|
No. of case-patients†
|
No. of deaths‡ |
Total case-patients |
Attack rate (%) |
|
Age group |
|
0-1 yrs |
55 |
24 |
15 |
39 |
71 |
|
2-5 yrs |
267 |
48 |
11 |
59 |
22 |
|
Male, No (%) |
188 (58.4%) |
31(43.0) |
13 (50) |
44 (44.9) |
23§ |
|
Tribe |
|
Bangro |
162 |
38 |
14 |
52 |
32 |
|
Nishing |
113 |
23 |
5 |
28 |
25 |
|
Sulung |
47 |
11 |
7 |
18 |
38 |
|
Overall |
322 |
72 |
26 |
98 |
30 |
* The population denominators were estimated based on following assumptions: (a) 13% of the total population is
under-fives (b) estimated number of infants= [Number of live birth- (No. of live birth X Infant mortality rate)]
where No. of live birth = birth rate of the area X total population of the area. Birth rate and Infant mortality
rate of the district during 2008 was 22/1000 population and 60/1000 live births respectively (c) sex ratio of the
district = 901 females: 1000 males (2001 census); †Suspected case-patients among those attending medical camps;
‡Deaths as reported by local health workers and local administration; §Attack rate in females 40%.
|
Discussion
A large outbreak of pertussis with high mortality
occurred in a remote district of Arunachal Pradesh during 2007. The
outbreak occurred due to low coverage of pertussis vaccine. The
administrative coverage of three doses of DPT vaccine in the district in
2007 was <5%(4). As per NFHS-3, the coverage of fully vaccinated children
in Arunachal Pradesh was only 28%(5). Difficult terrain, inclement weather
and all public health facilities not conducting fixed day immunization
sessions could be the reasons for low coverage.
During our investigation, we could not search for
case-patients in all villages because of the distances involved and the
inclement weather. Magnitude of the outbreak based on number of
case-patients who attended medical camp is likely to be an underestimate
of actual cases that might have occurred in the area. This could also be
the reason for lower attack rates observed during this outbreak, as
outbreaks in unvaccinated children are often associated with very high
attack rates(6).
Deaths due to pertussis, though rare, can occur due to
complications like pneumonia and encephalopathy. The disease could also be
fatal among infants, malnourished and unvaccinated children. In the
present outbreak, we did not calculate the case-fatality ratio as the
information about all pertussis cases in area was not available. However,
deaths of 26 under-fives in the area indicates severity of the outbreak as
well as inadequate management of the case-patients. A large proportion of
death among infants observed in this outbreak is comparable with the
disease epidemiology in pre-vaccination era(6).
Absence of laboratory confirmation was the main
limitation of our investigation. Non-availability of transport media and
long delay in transporting samples to the laboratory in Assam could be the
reasons for this. The case definition of cough of two weeks or more has
been shown to be both sensitive (84-92%) and specific (63-90%), and has
been suggested during outbreak setting(7). We used a more specific case
definition by including case-patients having other symptoms like
paroxysmal cough, inspiratory whooping and post-tussive vomiting among
under-five children, as well as included deaths that occurred among
under-fives. Thus, the clinical picture of case-patients and fact that
majority of them were among infants, indicate that the outbreak was due to
pertussis.
Based on these findings, we recommend establishing
facilities for conducting routine immunization in Sarli and organizing
special campaign in the area to vaccinate all under-fives with full course
of vaccines; educating the community about need for childhood vaccination;
and strengthening disease surveillance system in the district and making
available viral/bacterial transport media for common epidemic-prone
diseases, at the state laboratory.
Contributors: TT, DG and HT collected the data, TT
analyzed the data, and TT and MVM drafted the article. The final
manuscript was approved by all the authors.
Funding: None.
Competing interests: None stated.
|
What This Study Adds?
• An outbreak of suspected pertusis is reported
from Kurung-kumey, a remote district of Arunachal Pradesh.
|
References
1. World Health Organization. WHO-Vaccine preventable
diseases: monitoring system. 2006 global summary: WHO, Geneva, 2006.
Available at: http://www.who.int/vaccines-documents/GlobalSummary/GlobalSummary.pdf.
Accessed 10 March, 2009.
2. World Health Organization. WHO Recommended
Surveillance Standards. Second edition. WHO/CDS/CSR/ISR/99.2 Available at:
http://www. who.int/csr/resources/publications/surveillance/whocdscsrisr992.pdf.
Accessed 10 March, 2009.
3. Centers for Disease Control and Prevention.
Guidelines for the Control of Pertussis Outbreaks. Atlanta: Centers for
Disease Control and Prevention: 2000.
4. District Health Action Plan, 2007; Koloriang, Kurung
Kumey district: Office of District Medical Officer; 2007.
5. International Institute for Population Studies.
National Family Health Survey (NFHS-3) 2005-2006, India. Mumbai: IIPS;
2007.
6. Cherry JD. Pertussis in the preantibiotic and
prevaccine era, with emphasis on adult pertussis. Clin Infect Dis 1999;
28(Suppl 2): S107-111.
7. Patriarca PA, Biellik RJ, Sanden G, Burstyn DG,
Mitchell PD, Silverman PR, et al. Sensitivity and specificity of
clinical case definitions for pertussis. Am J Public Health 1988; 78:
833-836.
|
|
|
 |
|
